Kris Heinzman retweetledi

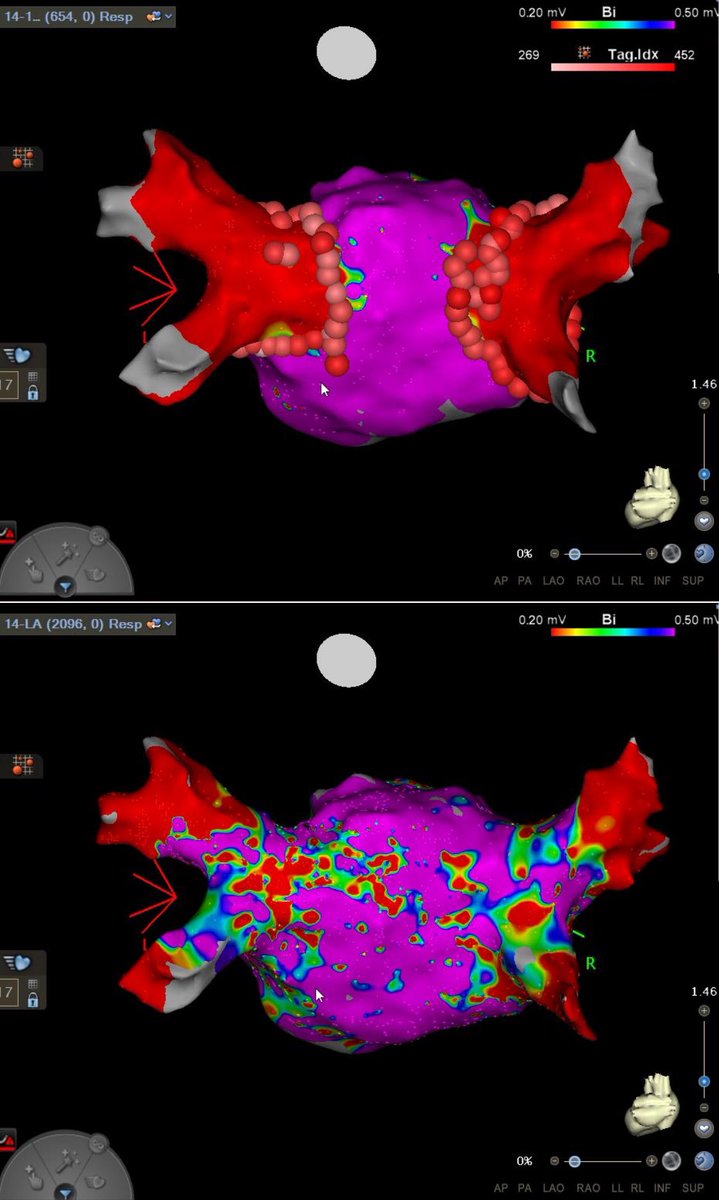
Is #PulseFieldAblation replacing RF Ablation?
Dr. Kristopher Heinzman & @pkothapalliMD explore its clinical promise, training risks & how EPs decide which patients fit PFA vs RFA.
Watch full video 👉 youtu.be/WyH-vpY65gU
#Cardiology #EP #Afib @HRSonline @HeinzmanSetonEP

YouTube
English