Nanda Iryuza retweetledi

@ISeropianMD @MichaelMegalyMD complete video: details of the clockwise rotation (the burr stretches and pulls the guiding Cath in the coronary)
English
Nanda Iryuza
441 posts


@Iryuza
Interventional Cardiologist at National Cardiovascular Center Harapan Kita 🇮🇩



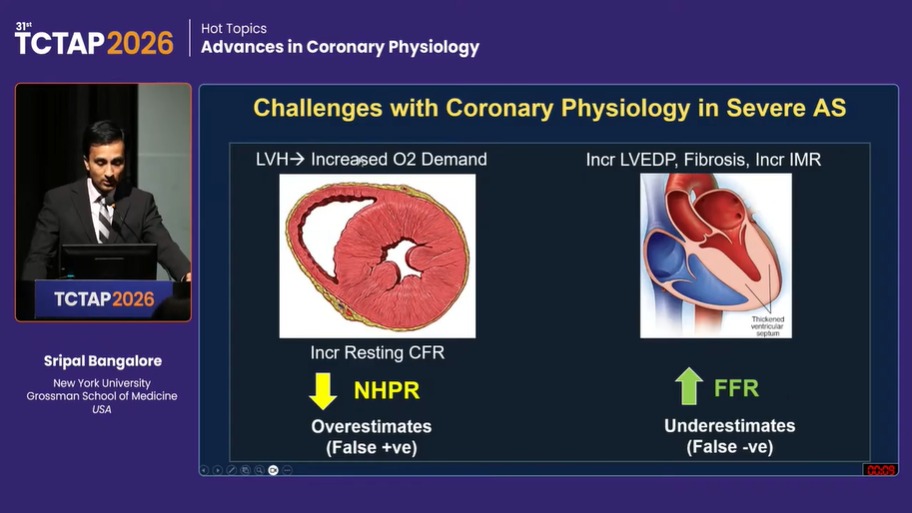
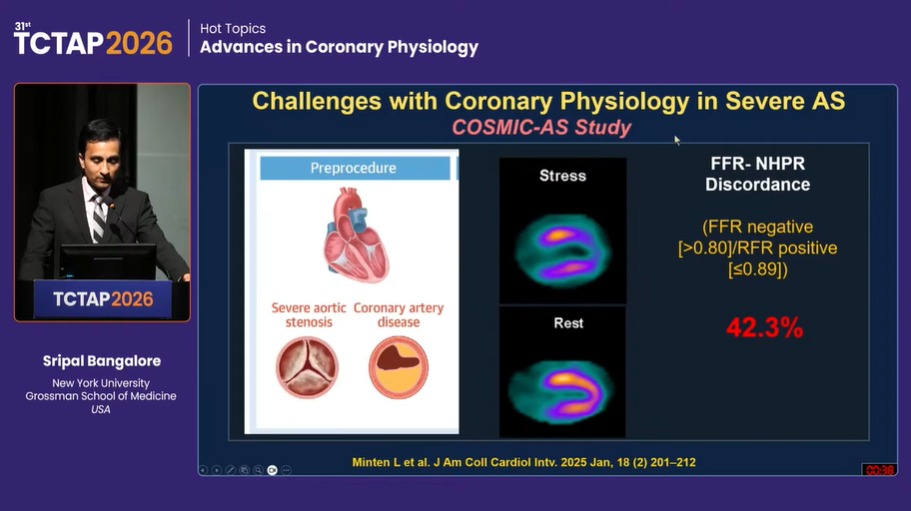


#TCTAP2026 ❤️🔥 Get ready to tune into a comprehensive coronary physiology session covering invasive & non-invasive tools—from FFR/NHPR discordance and MV testing to wire-based/wireless strategies, CT-FFR, and landmark trials; refining real-world decision-making in the cath lab.






“just look at the degree on that chick” And I’ll bag my fourth degree soon. Stay mad 🤍
















💡 Experience interventional cardiology like never before! Explore 𝘀𝗶𝘅 𝗱𝗲𝗱𝗶𝗰𝗮𝘁𝗲𝗱 𝗹𝗲𝗮𝗿𝗻𝗶𝗻𝗴 𝘁𝗿𝗮𝗰𝗸𝘀 — each designed to enhance your clinical expertise and elevate professional excellence. 📅 6–8 Nov 2025 | 📍 Shangri-La Hotel, Jakarta 🔗 Discover more at isicam.id More Information: Mrs. Santi: +62 813 1522 7958 🅾️ Instagram: @isicam_inalive @isic.or.id 🌐 isicam.id #ISICAM2025 #StayOnTrack @mmamas1973 @JEscaned @Laserrman @shaoliang_chen @rotamonster @Ditongaje @markzroland @fanisuslina #ISICAM2025 #StayOnTrack

1/ Most people think the heart drives circulation. But what if that’s backwards? Anderson’s model flips the whole idea of cardiac output on its head — and it changes how you think about fluid, flow, and failure. 🧵👇 #physiology #FOAMed #MedTwitter #criticalCare #cardiacOutput




