
Joe Silletti
186 posts
Joe Silletti
@JoeSilletti
Friend of Rufus the Dog, urologist.
Katılım Şubat 2019
174 Takip Edilen45 Takipçiler

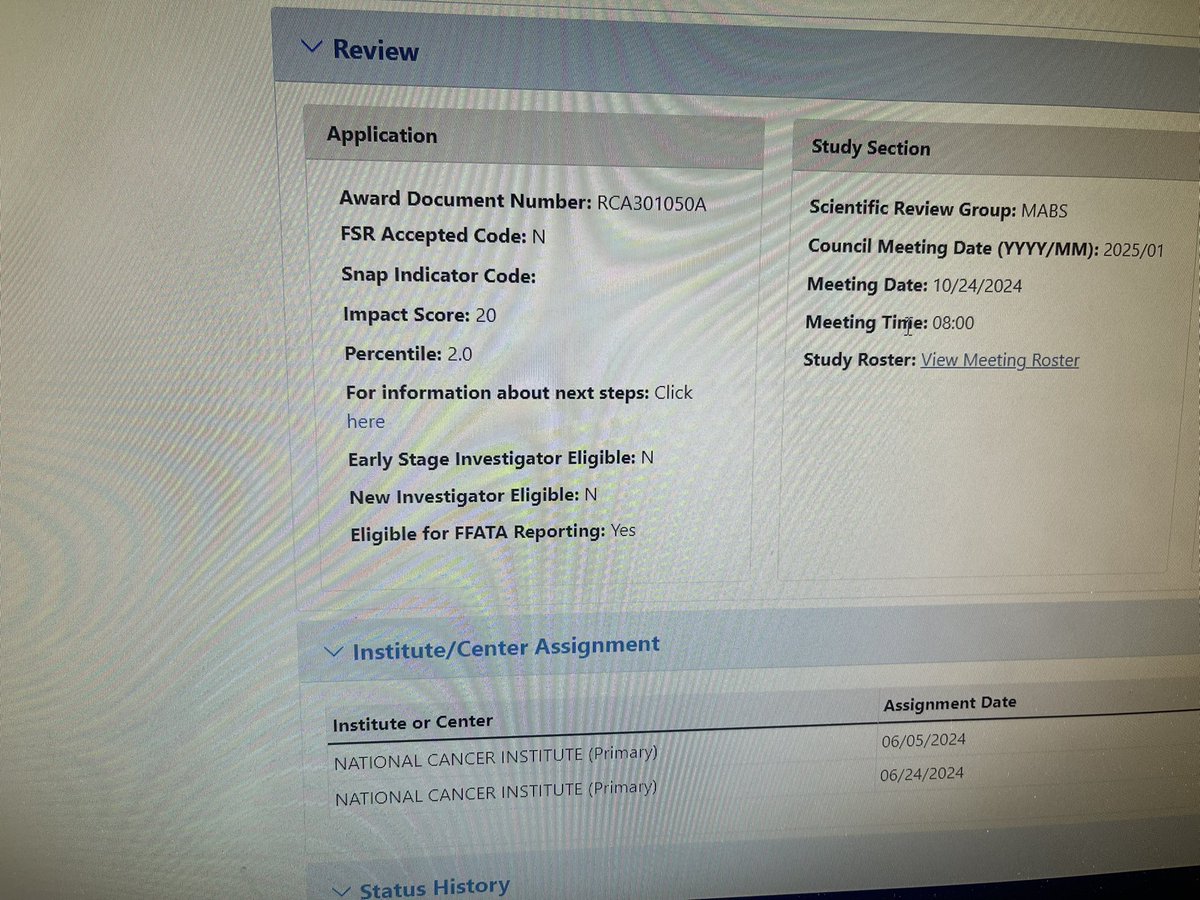
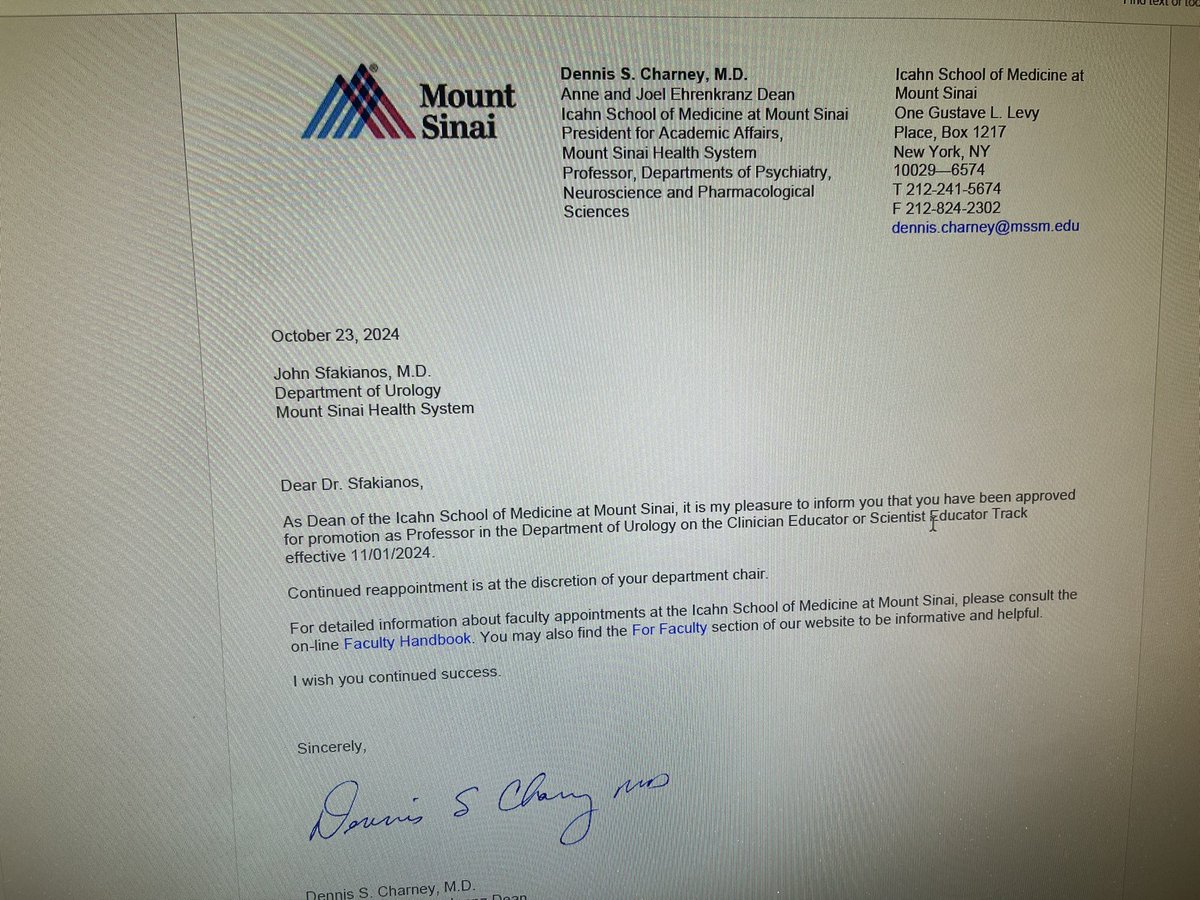
So blessed to have been Promoted to Professor and obtain a fundable score for our second R01. All this is only because I have been lucky enough to train with, collaborate with and just allowed to be around so many amazing individuals! Thank you to all of you! @MountsinaiUro
English
Looking for a robotics trained urologist to take over our established practice at Bronxcare. Reach out with any questions. #urologist #urology
English
@CanesDavid @tryheidi I love this. Efficacy leads to more productivity and better outcomes. Your error rates go down. This sounds like a win-win.
English

@SWilliams_MD @siadaneshmand Wait. So you just pull hard and ligate at the external ring??
English

@siadaneshmand Nice job and agree no longer open external ring aligns with internal but still get high ligation. No more opioids.
English

Pts should rarely require opioids post radical orchiectomy. This study puts its use into perspective. Don’t open the external ring! Significantly reduces pain and does not impact high ligation of cord or oncologic principles.
Alireza Ghoreifi, MD@alirezaghoreifi
Great study by @UroAlsyouf published in @UrolOncol ▶️2911 pts > PSM analysis 🎯Postop opioid prescription following radical orchiectomy is significantly associated with developing new persistent opioid use @TestesCancer @SUO_YUO 🔗authors.elsevier.com/c/1jXUy3r93ncs…
English
@EitanGlucksman Send me a CV at jsilletti@bronxcare.org and we can chat
English

@JoeSilletti How do I find out more about this opportunity?
English
@JoeSilletti By the way I wonder if med schools still teach that mystery novel approach? 🤔
English
☎️ A frame for residents calling the on call attending:☎️
#TipsForNewDocs
“I have a patient with ____ who I think needs ____”…
…and then comes the story.
👊 PUNCHLINE FIRST 👊
Why? This changes how the recipient listens, and the old med school model of unfolding a dramatic story leaving suspense for the eventual punchline should not exist.
Urology examples:
“I have a 78 year old with an infected 8mm UPJ stone who needs a stent”
“I have a 54 year old woman with a 3mm UVJ stone who I think we can send home”
👂The attending listens with intent to support or disprove your plan. It’s perfectly fine if the assessment or plan is wrong.
“Sure,” you say, “but this is July, and interns may not know what needs to be done!”
Agree- but taking a stab is the only way to learn. As @TedEdson1 taught me in 2001, “Be right or be wrong, but be something.”
So the frame can be:
“I have a 64 year old woman in the ER with a 6mm right mid ureteral stone and I am on the fence about whether we need to intervene”
Or, “We got consulted on incidental bilateral hydro in the ICU and I am unsure how to put it all together”
Bingo… now the attending listens differently.
{caveat— not all attendings will agree with this, and I’m sure they’ll tell us why 👇}
p.s. this should be the same frame for ER docs calling just about anyone
English
@_ToddBeane @NobletStrength I don’t know a lot about soccer. But from what I have seen, the difference between good and great players is not skill, but the ability to think quickly.
English

@NobletStrength Repeating the task of finding solutions in the challenging environment of context is exactly what I suggest to be most fruitful. 💥🕺🏼
(And a productive alternative to traditional training)
All the best.
#TOVO
Sant Pere de Ribes, España 🇪🇸 English

Ya, let's throw out over a hundred years of sport science understanding of skill development because Todd Beane has some doubts about it. This isn't even controversial, repeating a task and progressively making it more challenging absolutely improves technical skills.
English
@CanesDavid How about, the days after a vacation are not over booked as to “catch up” for time taken off.
English
I was asked what I would do to mitigate burnout. Here is my list.
What would you add?
🧯🔥🔥🔥🔥🔥🔥🔥
𝙳𝚊𝚟𝚒𝚍 𝙲𝚊𝚗𝚎𝚜@CanesDavid
😶 Typical response to mitigate burnout (all sincerely well intentioned): -create a wellness or serenity suite -free massages -appoint wellness officers and a committee -resiliency training -team building retreats -stress management workshops -recognition and reward programs -fitness memberships -healthy eating programs 😊 What’s actually needed are workflow improvements (much more difficult, high hanging fruit). 💡 We want doctors to be doctors, not transcribers or data entry technicians. 👍 We want them engaged in the most fulfilling 1:1 patient interactions at the heart of medicine. 😁 More face to face, less computer time. So this means: 🔵 everyone at top of license. Even consider expanding scope. E.g. what if RNs are allowed to refill chronic non-controlled meds without orders? 🔵 limit electronic “inbasket” messages to only the most critical. Perhaps normal values should not ever have to be signed off, for instance, unless MD herself flags it 🔵 using tech or personnel, notes should be skeletonized already so docs can focus on decision making, not data gathering 🔵 Patients should be primed with educational materials before they arrive, as a flipped classroom, because the 1:1 interaction is sacred and must not be wasted (I have COI on this one with @WellPrept but genuinely believe) 🔵 Using AI or human scribes, visit documentation should happen automatically (just like lawyers in court have stenographers) 🔵 if salaries are RVU based, then RVUs at the doctor’s run rate should be attributed to vacation weeks (otherwise, are they vacations?) 🔵 Vacation inbasket (or equivalent) coverage mechanisms, just like call coverage 🔵 allow for paid sabbaticals after X years of service 🔵 Eliminate or substantially curtail MOC 🔵 Extend recredentialing cycles to the max allowable by law, or change the laws to extend interval (BLS, laser recert, fluoroscopy recert, licensure cycles, etc) 🔵 remove prior authorization 🔵 offer flexible and part time schedules 🔵 automate any and all routine tasks
English
@CanesDavid Limiting PVP to prostates 80g or less seems short sighted. It’s safe and works well if one is patient.
English
It’s 2024, AI and machine learning are all the rage, 3D printers are now toys for children, and we are still reminding uros to
✅ know the prostate size before operating
😂 😶 😞 🫠
Ricardo R Gonzalez MD@RRGonzalezMD
Happy new year! Have y’all checked out the @JUrology @AmerUrological #BPH guideline update? #PAE and @iTind_System added for select patients. TUMT out. Important to know prostate size, patient goals prior to surgical interventions. Nice job Jaspreet Sandhu, Tim Wilt, @BladderBud et al. @SocietyofBPD #rezum #urolift #aquablation #holep #AEEP and more options to come! 🤩
English

NOTE: TOVO opens this coming week to public
Monterey, California Camp -->
tovoinstitute.com/monterey-resid…
Princeton, New Jersey Camp -->
tovoinstitute.com/princeton-resi…
About TOVO Academy -->
tovoacademy.com
About Todd Beane -->
toddbeane.com
Dallas, PA 🇺🇸 English
💥💥💥⚽️⚽️
Summer USA TOVO Programs
We have already received several applications for Monterey and Princeton.
Monterey, California
July 2-11
Princeton, New Jersey
July 23-Aug 1
If you have interest, please fill out an application to reserve a spot.
Dallas, PA 🇺🇸 English
@tomsan106 sometimes the element that is lost on critics of your approach is that this is not the idea that early coaching gives a kid a leg up. The kids learn is failure, trying, learning, failing again, and eventual success, and that process can be fun. They become resilient learners.
English

This is a parent interacting with their child helping them to develop the ability to focus his/her attention. Perhaps the most important skill for a child to possess which is learning how to learn. Without focused attention learning does not take place. This is playtime between and parent and child, something that there is not enough of all over the world. It just so happens they are using a ball as the tool. This interaction between child and parent is crucial for a child’s cognitive, emotional, social and physical well being. We should be celebrating a parent playing with their child since we know statistically a child will do much better in life because of it.
I hope you can see this is little to do with coaching and more to do with great parenting. Helping a child develop confidence, focused attention, memory, balance and coordination, are all good things parents should encourage.
English

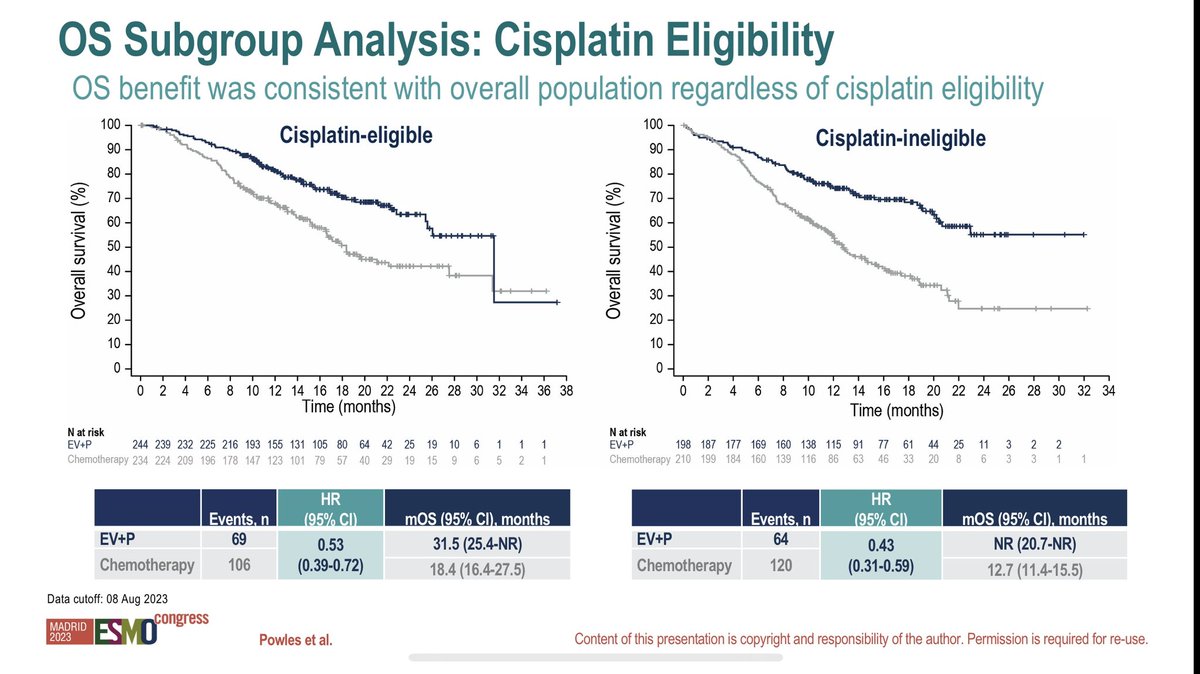
Enfortumab vedotin & Pembrolizumab improving PFS & OS by 55% & 53% respectively compared to platinum based chemo in 1st line UC (+avelumab in 30%). Chemo has not been beaten before (despite multiple efforts). RR and CR of 68% & 29% is hard to beat. DOR not reached (1/3)#ESMO2023



English
@FCAFigueiredo That’s bad outlet obstruction. Assuming no neurological issues such as DSD, he needs an operation.
English

BPH case of the week:
54y, moderate LUTS
USG, Prostate 29g, trabeculated bladder, PVR: 350ml
Cystoscopy: 🎥👇🏼
How would you treat him?
English
@drbrianwilliams @broadleaf_books It’s terrific. Finished it this weekend. Eye opening and tender. I was truly moved.
English

One more day until book launch and #TheBodiesKeepComing will be available in stores nationwide. A years-long journey is about to begin a new chapter. #authorlife #bookstoread

English

PSA: Don’t conceal carry your pistol in your pants pocket sans holster.
Sincerely,
Your friendly neighborhood urologist.
GIF
English