Sabitlenmiş Tweet

Mark Storey
4.2K posts

@ProtonStorey
Dr. Mark Storey MD - Radiation Oncologist. @OKProtonCenter. Background: #MDAnderson @VanderbiltU @BMESociety #RadOnc My blog: https://t.co/4S0MeQiWEI



6/ Radiology has PACS. Radiation oncology really does not. Our TPS does an amazing job planning dose. But we lack the hospital-wide communication layer that lets any clinician understand: What was treated? Where? To what dose? With what expected imaging change?

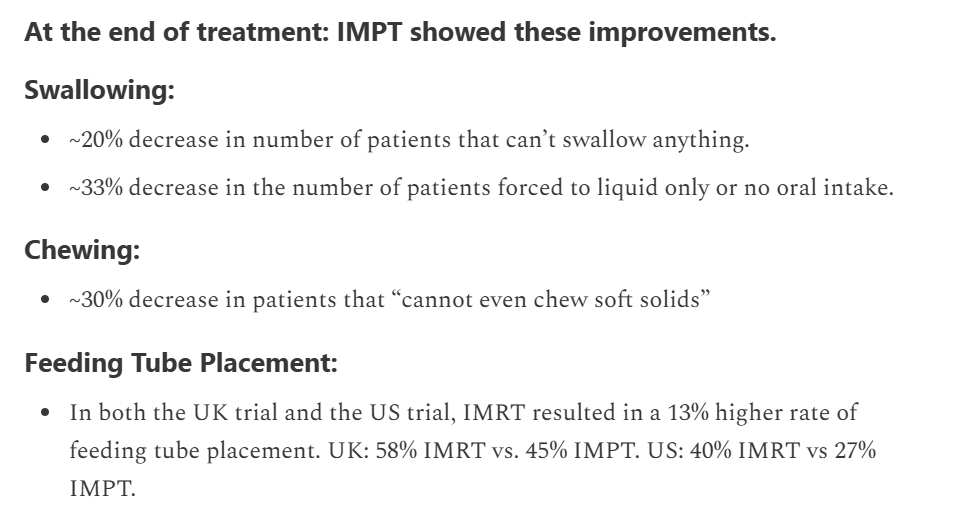
No QoL difference with IMPT vs IMRT in oropharyngeal cancer in the TORPEdO 🇬🇧 trial. How to explain the differences w/ @SJFrankMD 🇺🇸 trial? Planning? Patients? Crossover in the 🇺🇸 trial? Real absence of difference? Cc @EmmaHall71 @




@HimanshuNagarMD @piet_ost @SprakerMDPhD This is mostly STAMPEDE HR staged with CT Bone scan... And surely surprised by the results! Would love to see the effect cabazitaxel is having in sterilising micro mets.. Biological interaction? Food for thought!

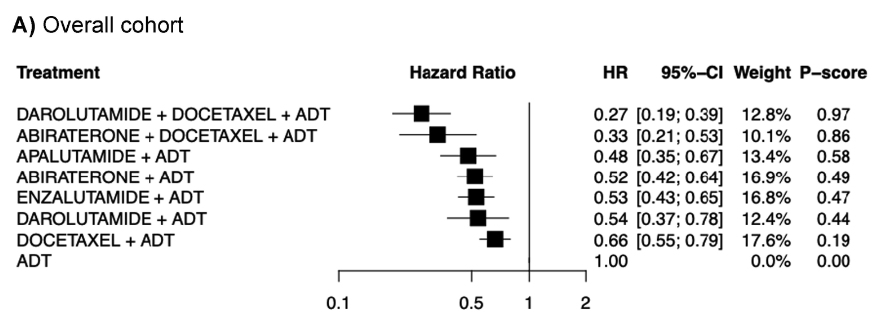
The #AUA26 advanced prostate cancer guidelines may be some of the clearest evidence of guidelines being influenced by bias and/or industry. EAU and NCCN recommend with consensus the use of RT to the primary in M1. EAU is “strong” evidence. NCCN is 2A, which is where most RCT data lands. AUA not only gives it grade C, but also conditional. That is where RWD lands usually. However, darolutamide doublet AUA gives grade A evidence despite only rPFS and no OS benefit. RT to primary showed OS benefit with or without docetaxel and an rPFS benefit with even triplet therapy in peace 1. STOPCAP confirmed robust PFS benefit of RT to primary. Unfortunate when “guidelines” are ways to push AUA or society members beliefs rather than facts. Not to mention the radonc on the AUA guidelines is amazing but Zietman is retired. Was told from AUA guideline authors that this 2026 update didn’t even circulate to all authors 🤔🤔 @ChadTangMD @HimanshuNagarMD @ndesai2005 @SbrtSean @Soum_Roy_RadOnc @TylerSbrt @PCaParker @jamesbyu @Prof_Nick_James @NehaVapiwala @fabiomoraesmd @aleberlin2 @DrAndrewLoblaw @I_Migowski @DrOmarMian @Alejogom @BobTimmermanMD @ASTRO_org

Cardiac Dose and Survival Outcomes Following Stereotactic Body Radiation Therapy for Primary and Metastatic Lung Tumors: A Substructure-Based Analysis - Advances in Radiation Oncology advancesradonc.org/article/S2452-…


Our letter to the editor in The Lancet critiquing the MD Anderson-led trial of protons v photons for OPC. Appreciate @SJFrankMD's well thought out response. I think we can all agree on two points: 1) Steve deserves major kudos for bringing level 1 evidence to the debate on protons v photons for OPC. These trials are extraordinarily difficult to run, and Steve, et al pulled it off. Well done! 2) Longer term follow-up from TORPEdO will help tease out the extent to which protons improves OS in OPC. @CJTsaiMDPhD @drlorenmell @xrtGenomics @DavidSherMD #radonc #hncsm thelancet.com/journals/lance…


Great value in side-by-side review of EAU and AUA prostate cancer guidelines in this new #AUA26 format. Good forum to review guideline methodology and reasons for discordance. Here @Tilki_De in session moderated by @Scarps_kristen
"AI has gotten better than radiologists at doing scans" I put @DarioAmodei's claim to the test by pitting a radiology resident against a state-of-the-art Chest X-ray AI Agent built by my colleagues led by @BoWang87. What do you think?


New in #practicalRO: Glowing Beauty: Collecting Uranium Glass—Dangerous Liaisons? #radonc tinyurl.com/promicke
