David Sher
1.9K posts


David Sher
@DavidSherMD
"Ultimately, the secret of quality is love. You have to love your patient, you to have to love your profession, you have to love your G-d." Avedis Donabedian




Day FOUR of #ESTRO26 Coverage by OncoAlert 🚨 Omission of elective nodal irradiation in HNSCC: long-term results and patient-level pooled analysis from 2 prospective trials (INRT-AIR & DARTBOARD) Presenter Sympascho Young 🇺🇸 A patient-level pooled analysis of 117 patients from two prospective trials (INRT-AIR and DARTBOARD) showed that omission of elective nodal irradiation for HNSCC was oncologically safe long-term, with a 0% rate of solitary elective nodal recurrence at 5 years. The trials used an involved nodal radiotherapy (INRT) approach assisted by an artificial intelligence model for detection of suspicious nodes. @DrSymYoung @DavidSherMD #RadOnc @ESTRO_RT @yasemin09896924 @LindaMrissa @christian_roenn @Valeriadionisi @gerryhanna @clchiang_hk @mtugceyilmaz @B_Tomasik @gmpetrianni @CiroFranzese1 @Atem84 @piet_ost @brachyexpert @BlanceS90 @The_PT_Explorer @BarbaraJereczek @Mat_Guc @ZilliThomas @AnnaKirby17 @PBlanchardMD @achoud72 Pinging OA faculty @MKnoll_MD @_ShankarSiva @Icro_Meattini @seanmmcbride @NiuSanford @nataliagandur @acampsmalea @to_be_elizabeth
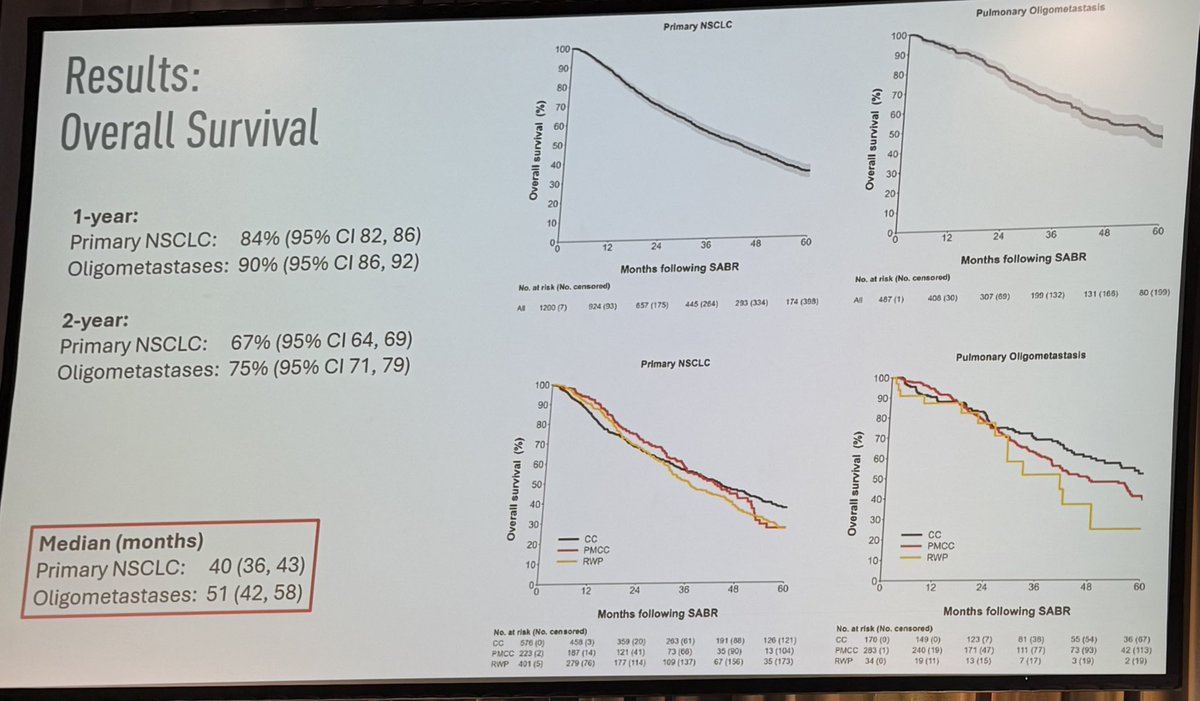
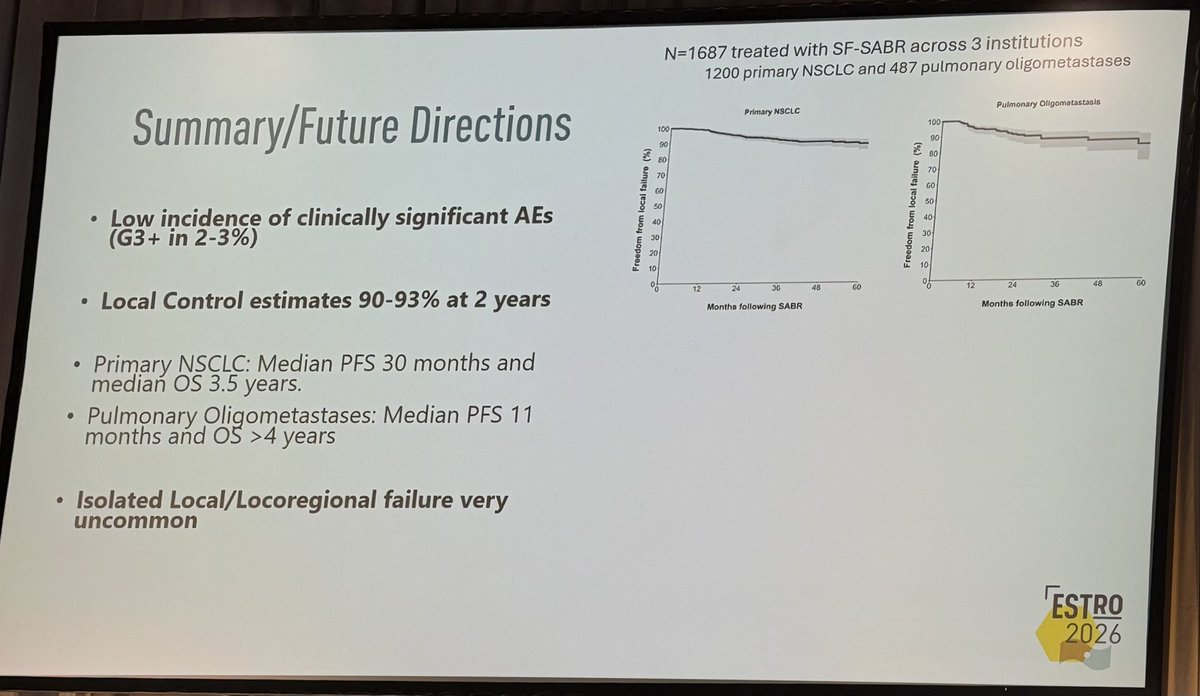
#ESTRO26 - 📣 FASTRACKII final results, median F/U of 5 years. Thank you patients, funders, investigators - #kidneycancer #kcsm 1) 100% Local Control: No local recurrences were observed at 36, 60, or 84 months. 2) 100% Cancer-Specific Survival 3) Grade 3 AEs remain at 10%




Day TWO of #ESTRO26 Coverage by OncoAlert 🚨 De-intensification of postoperative radiotherapy in HNSCC by omitting contralateral elective neck irradiation– long term outcomes of the DIREKHT trial Presented by Charlotte Frei 🇩🇪 #RadOnc ☢️ The DIREKHT trial is a prospective multicentre phase II trial investigating de-intensified risk-adapted radiation in patients with newly diagnosed, non-metastatic HNSCC after surgery. A total of 140 patients were included in the analysis. After five years, overall locoregional recurrence rate was 6.0% (95% CI [1.9; 9.9]). Cumulative incidence of locoregional recurrence was 3.0% (95%-CI [0.1; 5.8]). Details on recurrence patterns and dysphagia rates are presented at ESTRO 2026. @ESTRO_RT @yasemin09896924 @LindaMrissa @christian_roenn @Valeriadionisi @gerryhanna @clchiang_hk @mtugceyilmaz @B_Tomasik @gmpetrianni @CiroFranzese1 @Atem84 @piet_ost @brachyexpert @BlanceS90 @The_PT_Explorer @BarbaraJereczek @Mat_Guc @ZilliThomas @AnnaKirby17 @PBlanchardMD @achoud72 Pinging OA faculty @MKnoll_MD @_ShankarSiva @Icro_Meattini @seanmmcbride @NiuSanford @nataliagandur @acampsmalea @to_be_elizabeth


Day TWO of #ESTRO26 Coverage by OncoAlert 🚨 Five-year follow-up outcomes from JCOG1208: A single-arm confirmatory trial of IMRT alone for early-stage oropharyngeal cancer Presenter Satoaki Nakamura 🇯🇵 JCOG1208 prospectively evaluated intensity-modulated radiotherapy alone for patients with early-stage oropharyngeal cancer and favorable performance status. At five years, overall survival was 88% and local progression-free survival was 79%, with durable disease control after de-escalated treatment. These results support two-step IMRT alone as a treatment option that may reduce chemotherapy-related burden while maintaining favorable long-term outcomes. #RadOnc @ESTRO_RT @yasemin09896924 @LindaMrissa @christian_roenn @Valeriadionisi @gerryhanna @clchiang_hk @mtugceyilmaz @B_Tomasik @gmpetrianni @CiroFranzese1 @Atem84 @piet_ost @brachyexpert @BlanceS90 @The_PT_Explorer @BarbaraJereczek @Mat_Guc @ZilliThomas @AnnaKirby17 @PBlanchardMD @achoud72 Pinging OA faculty @MKnoll_MD @_ShankarSiva @Icro_Meattini @seanmmcbride @NiuSanford @nataliagandur @acampsmalea @to_be_elizabeth







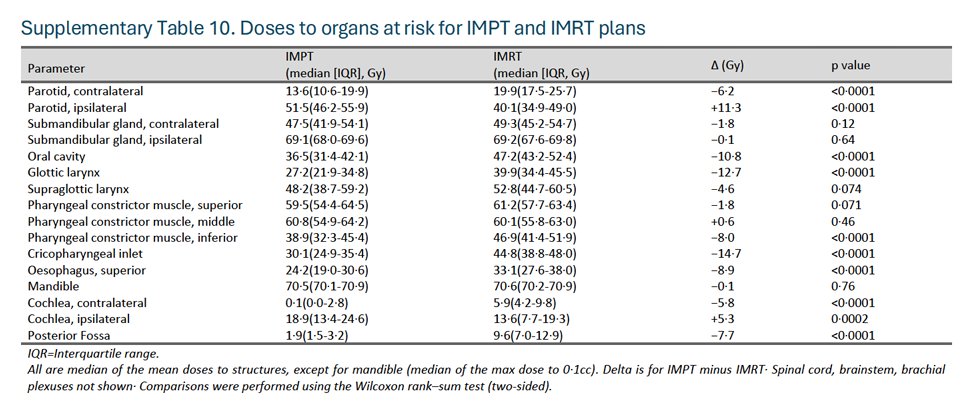
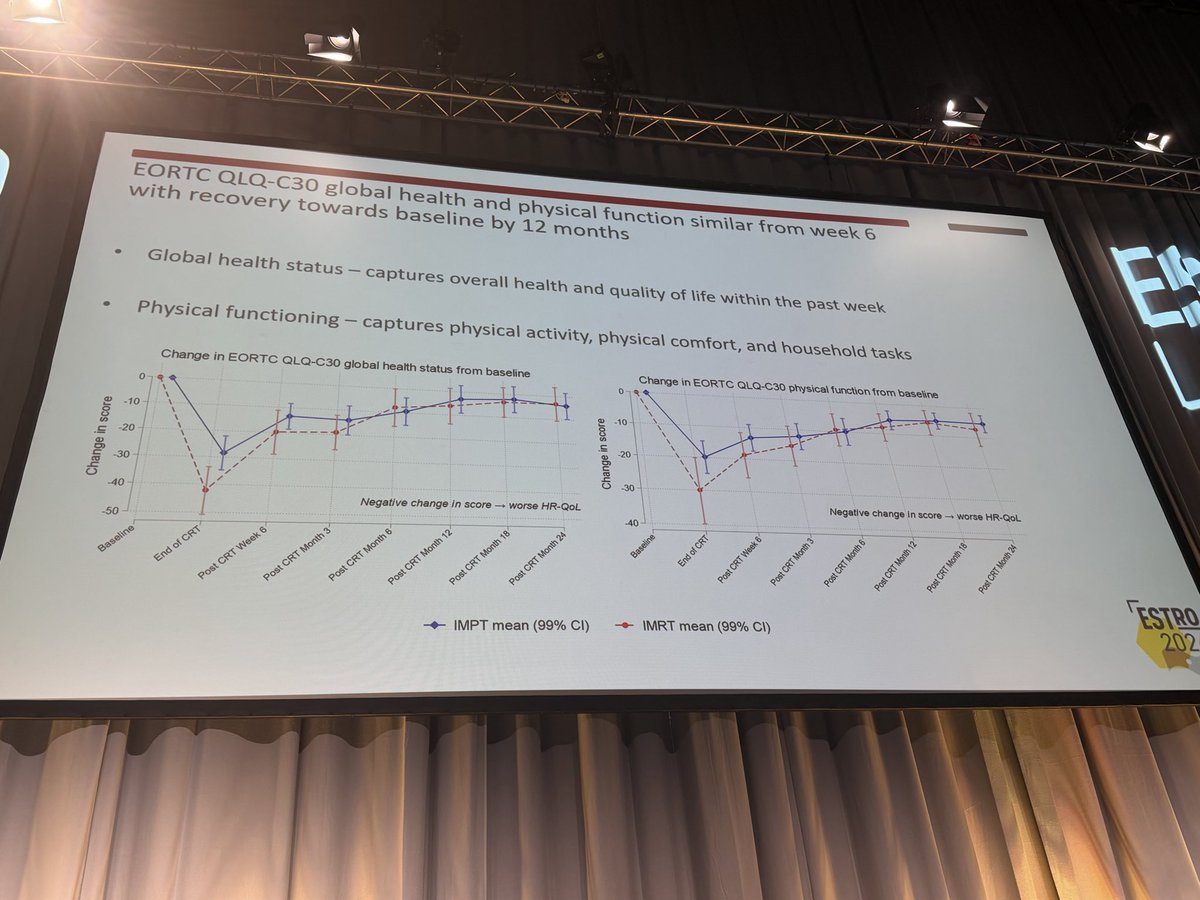
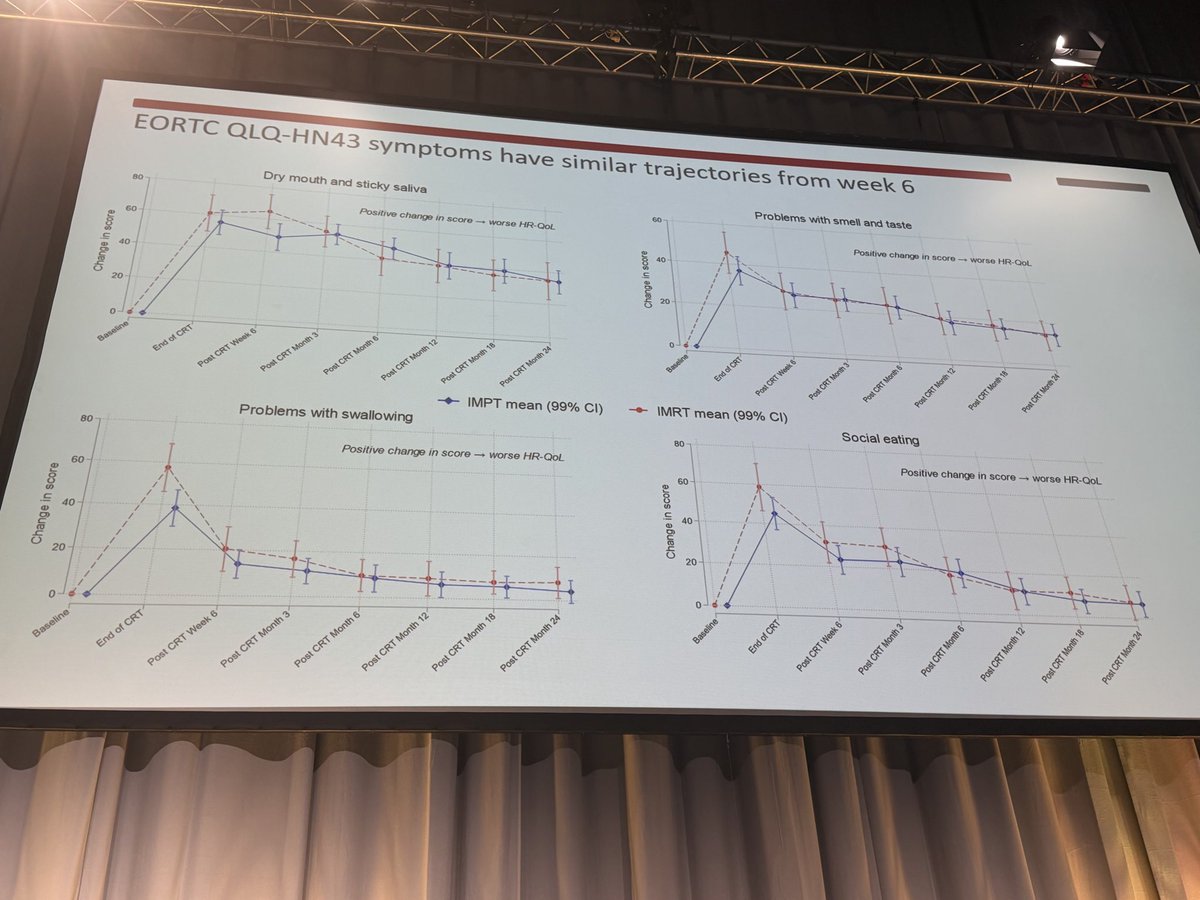
Our letter to the editor in The Lancet critiquing the MD Anderson-led trial of protons v photons for OPC. Appreciate @SJFrankMD's well thought out response. I think we can all agree on two points: 1) Steve deserves major kudos for bringing level 1 evidence to the debate on protons v photons for OPC. These trials are extraordinarily difficult to run, and Steve, et al pulled it off. Well done! 2) Longer term follow-up from TORPEdO will help tease out the extent to which protons improves OS in OPC. @CJTsaiMDPhD @drlorenmell @xrtGenomics @DavidSherMD #radonc #hncsm thelancet.com/journals/lance…


Sharing the results of ReACT 1.0 in @NatureComms -- the first study to use HPV ctDNA to guide CRT de-escalation in higher risk HPV+ OPC. ctDNA metrics may improve risk stratification. Grateful to our coauthors. @Naveris_inc @DanaFarberNews @jdschoenfeld1 nature.com/articles/s4146…