Iroh retweetledi

Hey @MrBeast, video idea for you: let's fix your Crohn's disease with diet. Give me 60 days. I know it is possible have seen MANY people reverse IBD (UC & Crohn's) with an Animal-Based diet or something like it.
English
Iroh
9.7K posts





Peter Misses the Plot: a Swift Debunking 👇 It’s come to my attention that @PeterAttiaMD has come out with an attempted debunk to The Cholesterol Code documentary and, more broadly, the research on lean mass hyper-responders. I won’t mince words: It’s embarrassing. It’s simultaneously arrogant, deeply misinformed, and, as I read it, a transparent avoidance of the facts at hand. It’s posturing, not insight. And I’m prepared to back that up. First, Peter attempts to discredit the documentary, the research on lean mass hyper-responders, and the Lipid Energy Model, on superficial grounds: credentials and authority. He almost exclusively referring to the work as a product of the Citizen Science Foundation (CSF), i.e., @realDaveFeldman: the 'uncredentialed' outsider. He conspicuously avoids discussing the broader teams involved, many of whom carry credentials that would easily meet the standards typically valued in more traditional, credential-focused settings (and exceed his own). Even setting aside myself, an MD-PhD, there is: Dr. Adrian Soto-Mota, MD-PhD, ith the Lundquist team, there are others who have co-authored work in this space, including Anatol Kontush, Ronald Krauss, William Cromwell, and, notably, Peter’s own former head of research, Bob Kaplan. Go figure. Might have been a fact fact for Peter to include: "My former head of research was a coauthor on the Lipid Energy Model paper I'm inadequately trying to debunk." And that’s the short list. I’ll also point out that when I was writing an editorial on lean mass hyper-responders, I reached out to Peter, and he declined to contribute, citing that it was not his area of expertise. He instead referred me to Ronald Krauss at “the expert,” who has now collaborated with us on a couple of projects. So even at a superficial level, what we’re seeing here is avoidance, posturing, and frank hypocrisy. Peter further attempts to cast doubt on lean mass hyper-responders by questioning the existence of the phenotype, which is, frankly, comical. It exists. It is defined by three clear cut points, and people meeting those criteria unquestionably exist. It is also a dynamic and reproducible phenomenon, as demonstrated by multiple experiments, case series, and even meta-analyses of randomized controlled trials that we have published. Peter forgot to talk about those data. No surprise there. Peter also demonstrates a misunderstanding of the Lipid Energy Model, for example by incorrectly suggesting a contradiction between the model and the low triglycerides observed in lean mass hyper-responders. And, more broadly, he reveals a lack of familiarity with the practical realities and constraints of clinical study design. If we are going to lean on authority, then it is fair to ask about experience. To my knowledge, Peter has not conducted clinical trials, and frankly, that gap shows here. At a deeper level, I don’t think Peter understands this physiology or this domain. And behavior like this, particularly when presented under the banner of scientific critique, is exactly the kind of thing that fuels “broader distrust in institutions and experts.” This is a textbook case of the pot calling the kettle black. I could go on, but I think the core point is clear. If further discourse is needed, Peter and his colleagues, including Tom Dayspring, have had ample opportunity to engage, collaborate, and discuss these ideas directly. If they choose not to, that speaks for itself. In the meantime, we’re not going anywhere. And no amount of pedantic posturing is going to change the trajectory of the data. Oh, and two more things… i. For those tempted to fall back on the overly simplistic take that “they’re saying high LDL is good” and “fear mongering about pharma,” or similar caricatures, you’ve entirely missed the plot. And, I have something coming this week. Again, if you interpret it as a pivot, you’ve missed the point entirely, as Peter has. ii. Finally, Peter’s central criticism seems to be that the documentary and our research suggest that even very high LDL cholesterol may not always indicate cardiovascular risk. Well, yes. The alternative is to argue that in all circumstances, at all times, very high LDL necessarily drives cardiovascular disease. This isn’t about discrediting, with a blanket statement, any role of ApoB or LDL in cardiovascular disease. This is about asking important questions at the frontier of science, because the status quo has been wholly inadequate in addressing the problem at hand. That's obvious. At least to some extent, we have been barking up the wrong tree. Anyone with a modicum of perspective can see that. And anyone with genuine curiosity would be willing to engage with the nuance, rather than lecture, avoid, and misrepresent, as Peter is doing here. Lastly: See the Cholesterol Code Documentary. It's on Amazon. And judge for yourself.



🚨 🚨 🚨OUR DOCUMENTARY IS HERE 🚨 🚨 🚨 🎥 Our film The Cholesterol Code dropped on Amazon! (Link next tweet) 🔥Personal stories of healing with keto 🔬New insights on Cholesterol 🫀Our groundbreaking study on heart disease 🙏 Please watch, share & leave an honest review! 🙏

🚨 🚨 🚨OUR DOCUMENTARY IS HERE 🚨 🚨 🚨 🎥 Our film The Cholesterol Code dropped on Amazon! (Link next tweet) 🔥Personal stories of healing with keto 🔬New insights on Cholesterol 🫀Our groundbreaking study on heart disease 🙏 Please watch, share & leave an honest review! 🙏
📺Gigantic Super LIVE Stream📺 for The #CholesterolCodeMovie ⏰ALL DAY TOMORROW starting at 8am PT ⭐️Featuring: 8 - Rob Kiltz - @doctorkiltz 8:30 - Emily Kaplan - @emilykaplanX 9 - Bret Scher - @bschermd 9:30 - Annette Bosworth - @AnnetteBosworth 10 - Ken Berry - @KenDBerryMD 10:30 - Nicholas Norwitz - @nicknorwitz 11 - Matt Baszucki - @matthewbaszucki 11:30 - Michelle Hurn - @MichelleHurnRD 12:30 - Stephen Hussey - @DrStephenHussey 1 - Philip Ovadia - @ifixhearts 1:30 - Robyn R Dobbins - @robynrdobbins 2 - Eric Rodgers - @DrEricRodgers 2:30 Eric Westman - @drericwestman





"When people are at their peak frustration, that's when they finally compromise, and it gets done," @Ripple CEO @bgarlinghouse tells @JaxAlemany on his optimism for passage of the CLARITY Act. "I think we're there."







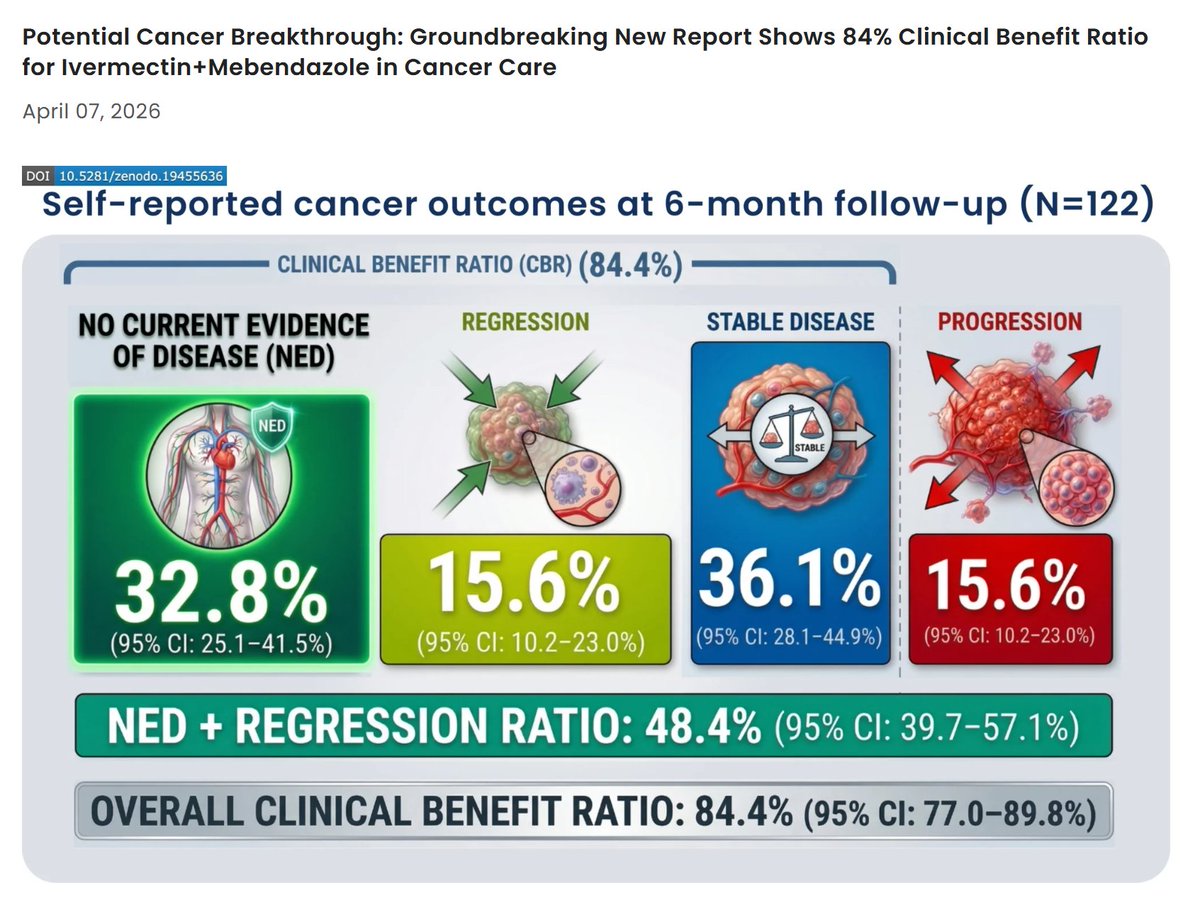
🚨BREAKING: Largest Real-World Study of Ivermectin + Mebendazole in Cancer Patients Shows 84.4% Clinical Benefit — Nearly HALF Report Cancer Disappearance or Tumor Regression After just 6 months, 48.4% of cancer patients taking ivermectin and mebendazole reported NO EVIDENCE OF DISEASE (32.8%) or tumor regression (15.6%), while 36.1% reported disease stabilization⬇️ We have completed the largest real-world human analysis to date evaluating ivermectin and mebendazole in cancer patients—and the results represent one of the most compelling clinical signals ever documented for repurposed anti-parasitic therapies in oncology. The groundbreaking analysis was made possible through a unique collaboration between The Wellness Company, the McCullough Foundation, and the Chairman of the President’s Cancer Panel (Dr. Harvey Risch)—uniting real-world clinical data, frontline medical experience, and high-level epidemiologic expertise to deliver urgently needed insights in oncology. This was a real-world prospective clinical program evaluation of 197 cancer patients, with 122 completing a follow-up survey at about six months (61.9% response rate). Cancer patients were prescribed compounded ivermectin–mebendazole, with each capsule containing 25 mg ivermectin and 250 mg mebendazole—most commonly taken at 1–2 capsules per day. The cohort represented a clinically relevant population, including a wide variety cancer types, with 37.1% of patients reporting actively progressing disease at baseline and many having already undergone chemotherapy, radiation, and surgery. At six months, 84.4% of cancer patients reported clinical benefit (Clinical Benefit Ratio: 84.4% [95% CI: 77.0–89.8%]): ✅ 32.8% reported no evidence of disease (95% CI: 25.1–41.5%) ✅ 15.6% reported tumor regression (95% CI: 10.2–23.0%) ✅ 36.1% reported stable disease (95% CI: 28.1–44.9%) Treatment adherence was high, with 86.9% completing the full protocol and 66.4% remaining on therapy at six months. The regimen was well tolerated, with 25.4% reporting side effects, primarily mild and gastrointestinal, and over 93% continuing treatment despite these events. Patients were treated in real-world conditions alongside concurrent therapies, including chemotherapy (27.9%), radiation (21.3%), surgery (19.7%), supplements (49.2%), and dietary modification (37.7%), supporting use as an adjunctive approach. Together, these findings represent a large, internally consistent real-world clinical signal that supports URGENT further investigation of ivermectin and mebendazole as low-toxicity, adjunctive cancer therapies. Given the strength of the signal observed here, advancing this line of investigation is no longer optional—it is necessary. This is NOT the end. We will continue advancing this work with larger datasets to further define and validate the role of anti-parasitics in cancer outcomes. The manuscript is now available as a preprint on the Zenodo research repository, operated by the European Organization for Nuclear Research, while undergoing peer review at leading oncology journals: “Real-World Clinical Outcomes of Ivermectin and Mebendazole in Cancer Patients: Results from a Prospective Observational Cohort.” @twc_health @McCulloughFund @P_McCulloughMD @DrHarveyRisch @DrKellyVictory @jathorpmfm @drdrew @PeterGillooly @FosterCoulson