Sabitlenmiş Tweet

Very proud and fortunate to be mentored by Dr. Neugut, who won the @columbiacancer Mentor of the Year Award


English
Connor Kinslow, MD
1.1K posts
@RadOncConnor
Passion for cancer research and clinical oncology. Radiation Oncology at MSKCC. #CancerOutcomes #NeuroOnc #CancerMetabolism




Remember when everyone said AI was going to completely replace radiologists? Dario Amodei just broke down exactly why that hasn't happened yet and what it means for the future of your career. Instead of wiping out the job, AI just ate the highly technical part (reading the scans), forcing humans to pivot entirely to the "human touch" (patient care). Amodei believes we need to adapt to AI step-by-step as it evolves. However, he didn't sugarcoat the endgame: he admitted it is highly likely that AI will eventually beat us at everything, including physical robotics.

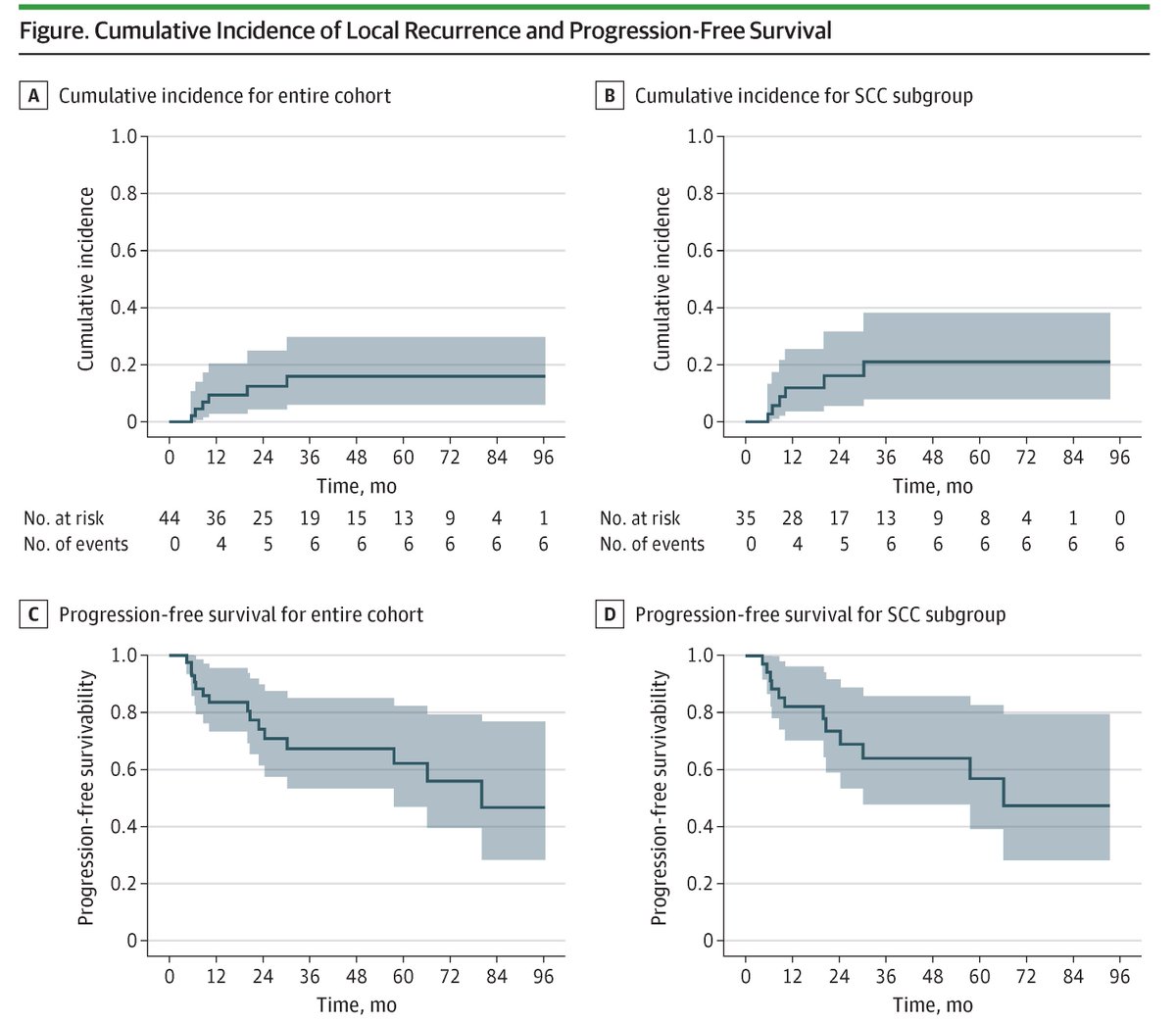




Cancer-Specific Mortality in Rare Histological Subtypes of Prostate Cancer: Radical Prostatectomy Versus Radiation Therapy link.springer.com/article/10.124… Study analyzed cancer-specific mortality in 427,055 #ProstateCancer patients with five histological subtypes, comparing radical prostatectomy (RP) versus radiation therapy☢️(RT) using SEER data (2004-2020). Results showed RP significantly reduced mortality in acinar, ductal, and neuroendocrine carcinomas, with five-year survival rates consistently higher than RT. However, no survival differences were observed between RP and RT for mucinous and signet ring cell adenocarcinomas, suggesting treatment selection should consider histological subtype. @carosiech @mario_dea_ @DrShariat @Albert0Briganti @OncoAlert 🚨 @Silke_Gillessen @AOmlin @weoncologists








🚀 Milestones achieved for VIGOR (EORTC‑2427‑BTG)! The first site is activated and the first patient has already been randomised in this Phase III study evaluating vorasidenib for IDH‑mutant astrocytoma. A strong start for this international effort. 🔗 eortc.org/blog/2026/01/2…