Rubab Aftab retweetledi
For rad oncs taking oral boards soon, here is a video I made a year ago to help prep for the GI section.
Good luck🍀!
m.youtube.com/watch?v=G157j6…
English
Rubab Aftab
382 posts

@Rubab_Aftab
Clinical Oncology Registrar |Co-Chairs of the Oncology Registrars' Forum, RCR| Fairer Training Leadership fellow|E=mc2 -an intuition | views my own
High-risk prostate cancer: what patients and physicians should know in 2026 Definition History Workup Management youtu.be/yLYcZzLbINQ





2025 approvals: Summary of 8 new drugs/indications in GU malignancies by @US_FDA 1. #Lu177 2. #Durvalumab 3. #Darolutamide 4. Intravesical #Mitomycyin & #Gemcitabine (TAR200) 5. #Enfortumab + Pembro 6. #Niraparib 7. #Rucaparib #gusm #OncTwitter #MedTwitter



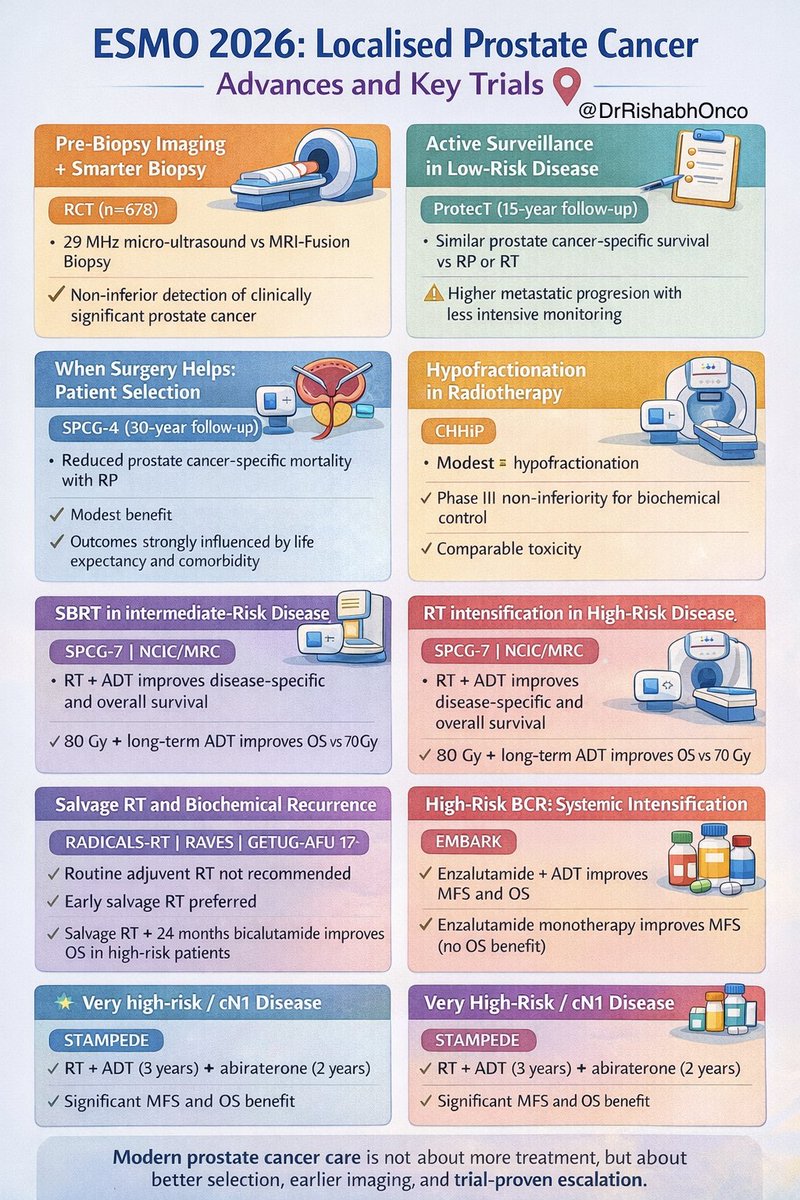

Is that time of the year again!…The ESMO preceptorship on prostate cancer in beautiful Lugano @myESMO