
@dgermain21 Yeah more confused about the biological rationale for Len in GCB than advocating for Ven in next gen trials
English
Sean Corcoran, MD PhD
819 posts

@S_Corcoran
PSTP Medicine Intern at Cedars-Sinai. MD @bumedicine. PhD @Cambridge_Uni and @theNCI via @NIHOxCam. Cancer Biologist. This is not my LinkedIn.

Im also not sure why the rationale would be that GCB patients would benefit from lenalidomide rather than maybe BCL2 inhibition etc. There aren’t many IRF4 positive GCBs!
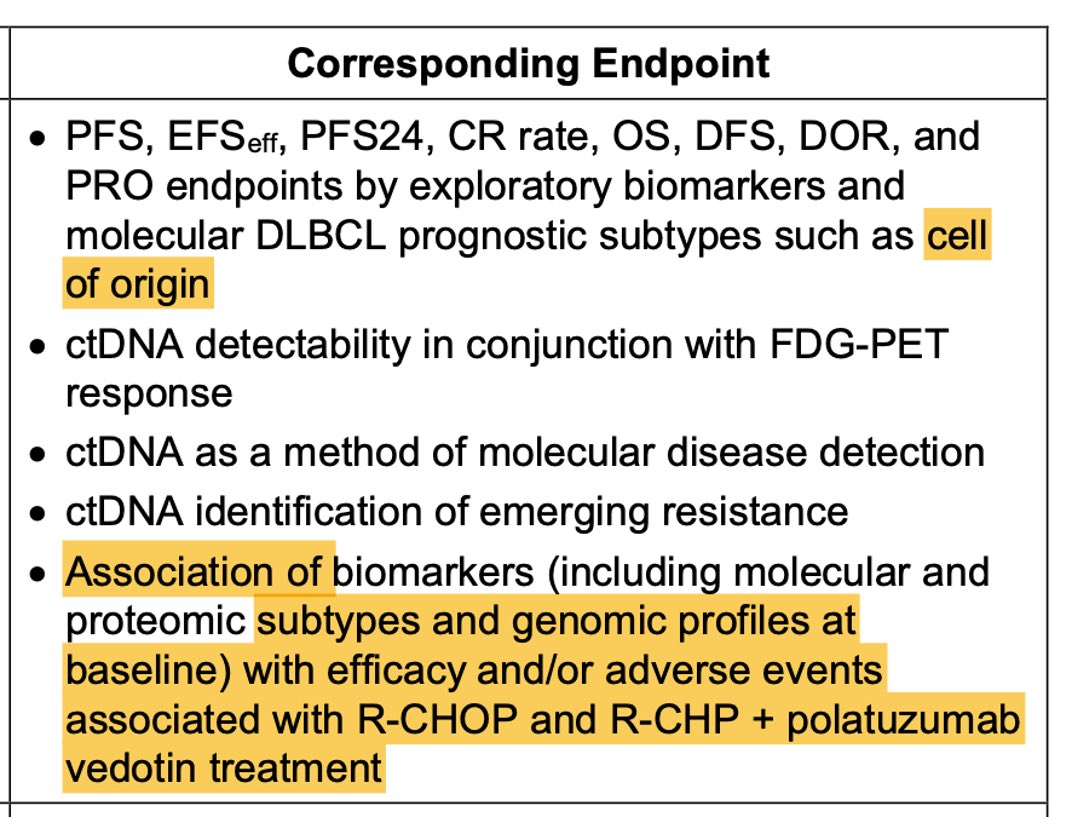
For frontMIND results DLBCL #lymphoma there seems to be a lot hanging on idea that Tafa Len has positive impact in GCB subtype & might be prioritized there - despite non-significant difference there in comparison to ABC where there was clear difference evident w/fewer pts #ASCO26


@lymphomahub ABC dominated responses with higher Gr3/4 neutropenia and thrombocytopenia

These Spencer Pratt videos by @dsonoiki are better than 99.9% of political consultant ads. He does it again.

I used to be a vocal skeptic of Hans and a key GEP fan, some say as an OG for GEP. I used to lament Hans IHC as the only tool available for my patients, when many trials used GEP instead. But I have been surprised by learning how IHC has dramatically improved over the last decade or so with availability of standardized antibody clones, use of auto strainers, and interpretation consistency. How was I convinced? We did a systematic meta-analysis of >2200 patients from 19 studies. We used the PRISMA diagnostic test accuracy framework for comparing Hans to GEP. library.ehaweb.org/eha/2026/eha-2… Remarkably, this analysis now clearly shows that Hans is consistently non-inferior to GEP across current modern studies at a 10% NI margin for Accuracy, Precision, and Specificity. This solid performance of Hans IHC is very much in line with current CAP benchmarks for diagnostic tests, and within the margins of NanoString GEP using FFPE vs original frozen GEP as the original elusive gold standard. Long live Hans as the best currently available SOC for COO across the globe.

MIT president: Why so many optimistic scientists are losing heart statnews.com/2026/05/27/sci… via @statnews









Don’t believe Internet fearmongers. @HHSGov defends public health AND supports medical freedom — period. HHS action … ❌ Does NOT pave the way for a new mRNA vaccine ❌ Does NOT provide Big Pharma with new, limitless protections from liability ❌ Does NOT allow for mandates of ANY kind ❌ Does NOT apply to any other medical products ❌ Does NOT apply to vaccines HHS action … ✅ Facilitates expanded access of favipiravir — and favipiravir ONLY — to treat hantavirus ✅ Allows individuals possibly exposed to Andes virus to access this drug ✅ Only covers VOLUNTARY administration and use — NO mandates ✅ Provides protection for a VERY LIMITED TIME, through July 18, 2026
Until now, physicians using AI in clinic had to assemble the patient’s context themselves. Allergies, comorbidities, medications, prior procedures, copy-pasted in from the chart. Today we’re announcing a partnership with @CedarsSinai. OpenEvidence now works directly inside Epic, drawing on the patient’s full record and interpreting the medical literature through the lens of that specific patient. Cedars-Sinai is the first academic health system to deploy patient-aware clinical intelligence at enterprise scale. The clinician asks a complex question in natural language. The answer reflects both the best available evidence and the patient in front of them. Patient data is never stored after the clinical session or used for any other purpose.