Samar Aboulenain retweetledi

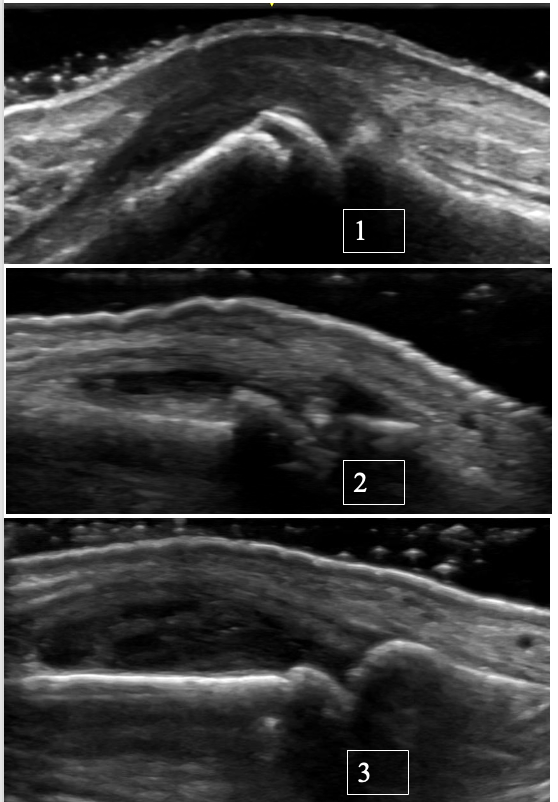
Ultrasound of the MCP joint with osteoarthritis and possible superimposed CPPD 👇
Ultrasound is a valuable tool for distinguishing between OA, CPPD, and inflammatory arthritis at the level of MCPs.
Case:
72-year-old right-hand-dominant retired carpenter presents with R MCP 3 pain and stiffness that has been intermittent over the past several years, worse with activity and has recently progressed with associated swelling.
Features suggestive of OA:
• Typically, no significant synovial hypertrophy. Effusions are more common
• Osteophytes are seen rather than erosions
• A “hook-like” osteophyte on X-ray or ultrasound should raise suspicion for superimposed CPPD
--> Ultrasound also enables precise targeting of small fluid collections for diagnostic aspiration.
Recommended reading:
Cipolletta E, Di Matteo A, Smerilli G, et al. Ultrasound findings of calcium pyrophosphate deposition disease at metacarpophalangeal joints. Rheumatology (Oxford). 2022;61(10):3997-4005. doi:10.1093/rheumatology/keac063
#MSKUS #RheumUS #CPPD #osteoarthritis
English