Sabitlenmiş Tweet

Pedro Graziano Sanchez
16.6K posts

@wikimagen
Cardiologist Cardiovascular Imager









Clinical features of adult patients w isolated #pulmonary_valve_endocarditis doi.org/10.3390/microo…


















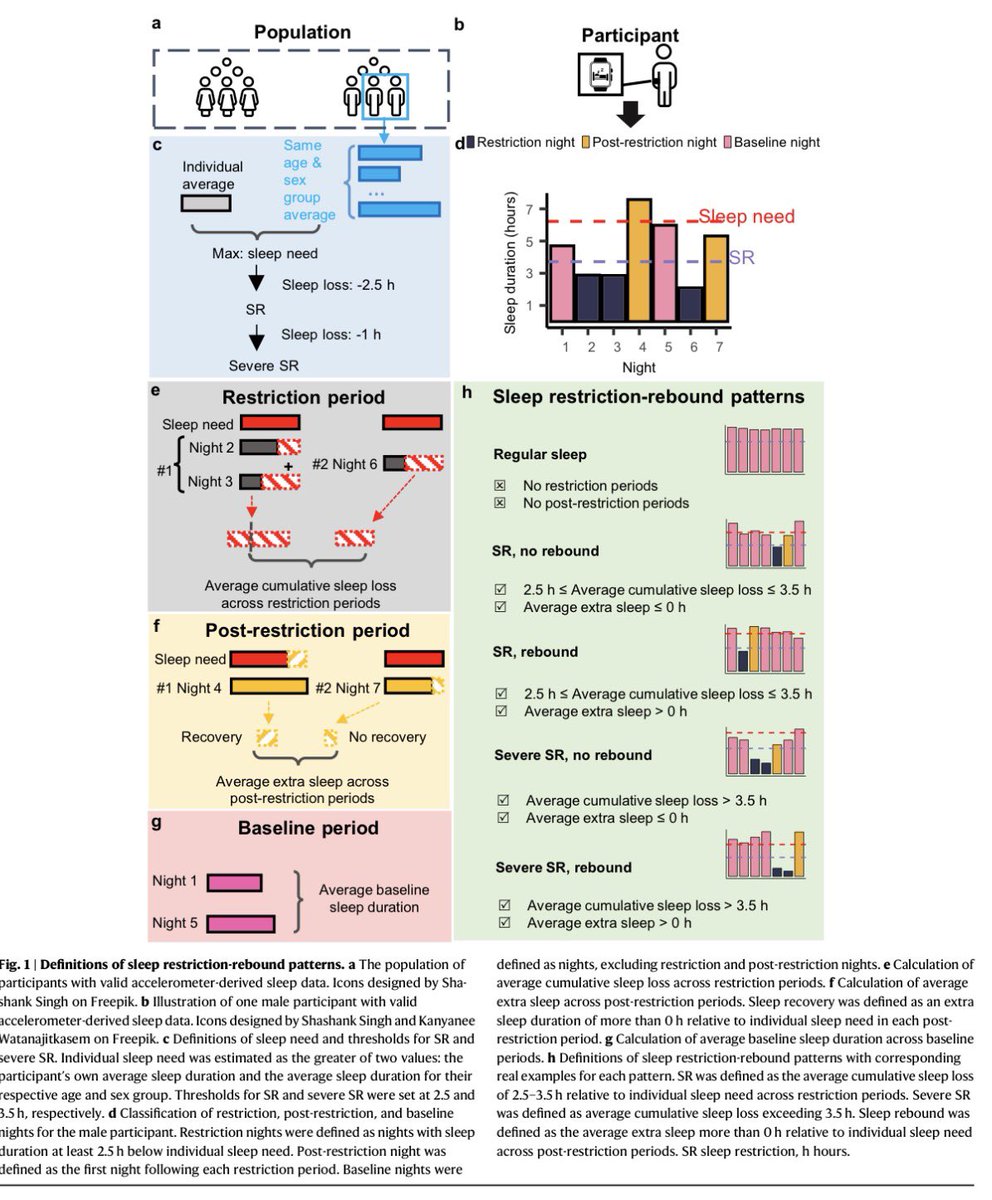
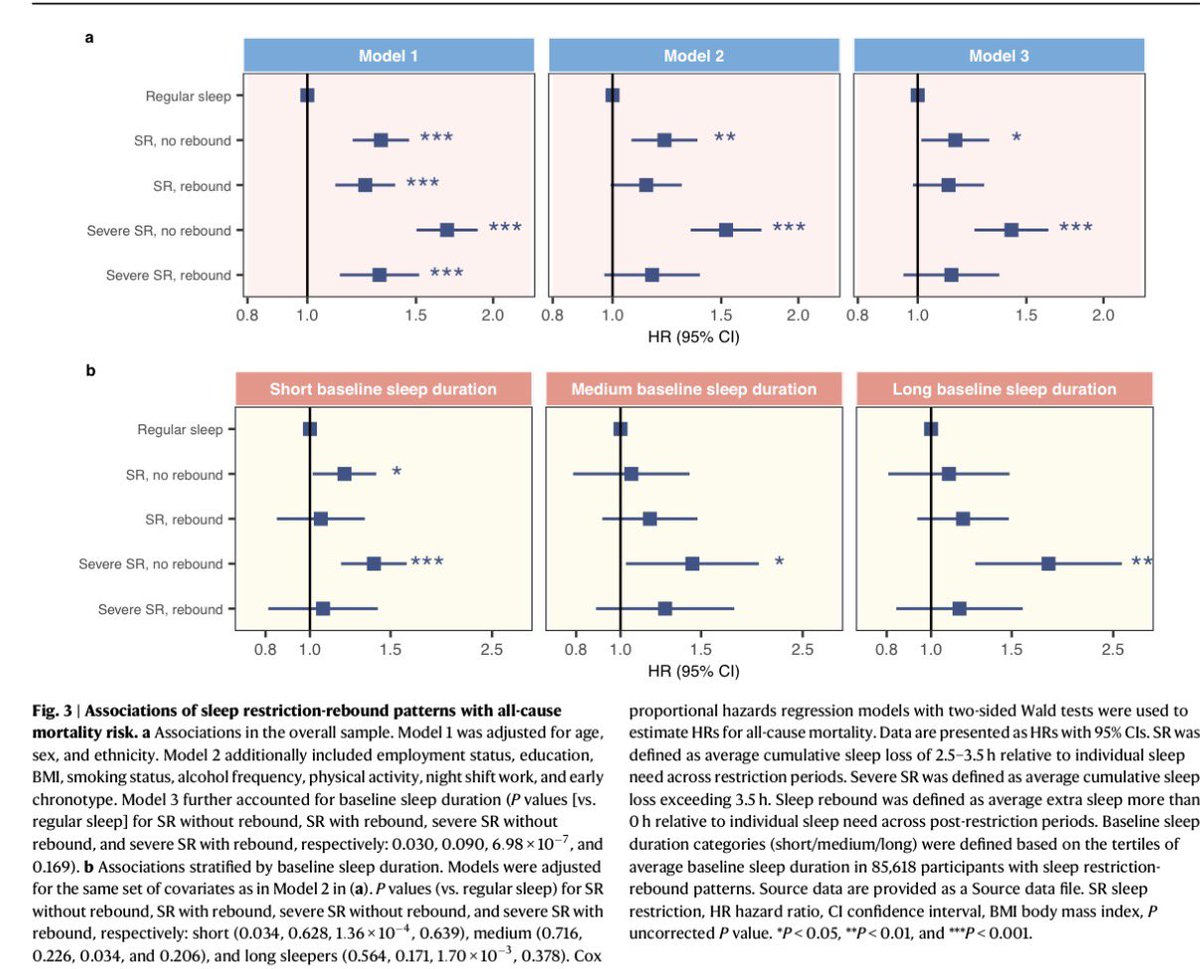
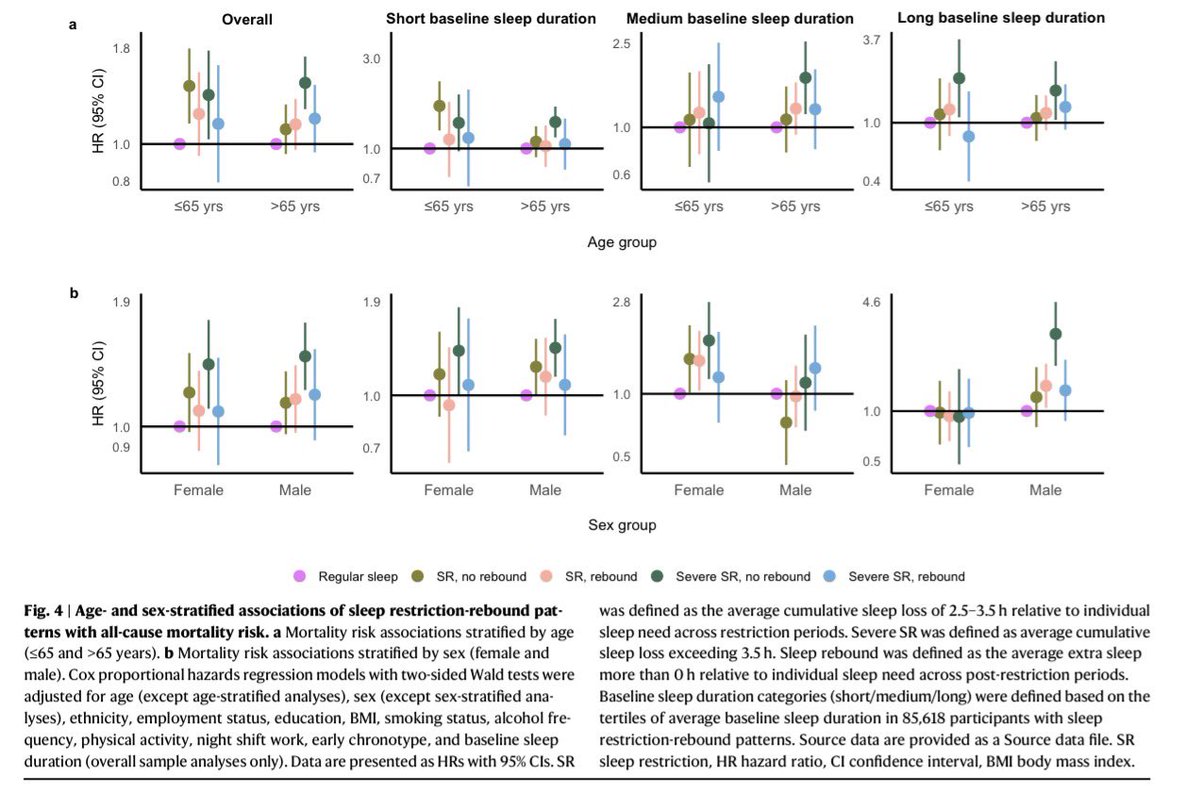
Uyku borcunu ödemek -yani, uykusuz kaldığınız günün ertesi günü daha fazla uyumak- uykusuzluğun getirdiği ölüm riskini telafi ediyor*.