Shashi Iyengar | Metabolic Health India®@shashiiyengar
🚨 Just Released: 10 Years of T2D Remission! 🚨
It is now part of the scientific record.
The study documents medication-free remission over a decade, achieved using a low-carbohydrate, lacto-ovo vegetarian diet, with systematic long-term safety evaluation.
To our knowledge, this is the first such study conducted globally.
What makes this work unique is not just remission, but rigour and duration.
For most of this period (approximately 70-75%), I followed a ketogenic diet; during the remaining time, I followed a low-carbohydrate diet with carbohydrate intake below 100 g/day.
This is a prospective N-of-1 longitudinal study, followed for a full decade, with repeated assessments across multiple domains:
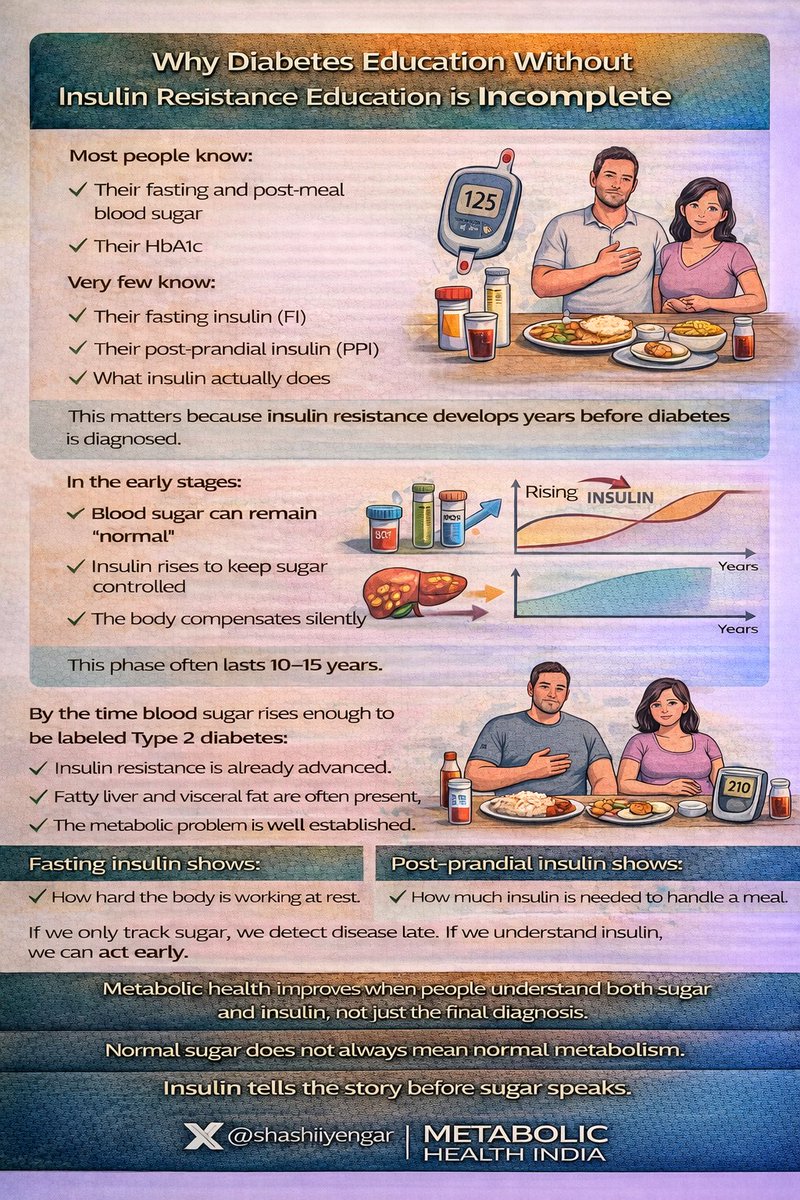
•Glycaemic control (HbA1c, fasting glucose, CGM) 🩸
•Insulin dynamics 🧬
•Advanced lipids including ApoB and Lipoprotein(a)
•Inflammatory markers 🔥
•Liver and renal function (including cystatin-C)
•Serial coronary artery calcium scans 🫀
•CT coronary angiography 🫀
•Carotid imaging (CIMT)
•Bone mineral density (DEXA) 🦴
•Detailed ophthalmic imaging 👁️
Starting Hba1c was 7.2%. FBS 152 & PPBS 253 mg/dl.
Achieved remission in the 4th month with Hba1c of 5.2%
Over 10 years:
•HbA1c, FBS & PPBS remained consistently in the non-diabetic range
•Average Hba1c was 5 in 10 years. (4.7 to 5.3)
•Average LDL and ApoB remained higher than recommended, but stable
•No microvascular complications
•No macrovascular disease
•No deterioration in renal, skeletal, or ophthalmic health
This was achieved without diabetes medication.
Importantly, this is an Indian study.
The dietary pattern was:
•Low carbohydrate
•Lacto-ovo vegetarian
•Culturally adapted
•Sustained for 10 years in a South Asian individual with the MONW (Metabolically Obese Normal Weight) phenotype
This directly addresses a major gap in the literature:
the absence of long-term, real-world safety data for low-carbohydrate approaches in South Asian, predominantly vegetarian populations.
It demonstrates that:
•Long-term remission is possible
•Sustainability over a decade is possible
•Comprehensive safety monitoring is feasible
•Replication at larger scale is testable
The intent of this work is not to prescribe, but to inform, challenge existing assumptions, and invite replication.
As an N-of-1 longitudinal study, these findings are not generalizable by design.
They are hypothesis-generating and intended to inform larger, prospective cohorts.
India carries one of the highest diabetes burdens globally.
Evidence addressing sustainability must emerge from within this context.
This study is now part of the scientific record.
Big thanks to Dr Jasmeet Phd @jasmeet481, whose relentless effort and scientific rigour made this study possible. She invested enormous time and care in shaping the manuscript and strengthening it to publication standard.
Grateful to my guru, Anup Singh, who introduced me to low-carb nutrition in 2015 at the time of my Type 2 diabetes diagnosis. His guidance laid the foundation for my 10-year low-carb journey.
Thank you to Arun Kumar who helped me when I was newly diagnosed.
Big Thanks to the 3 doctors who were part of my 10 years journey & are the co-authors also.
Dr Sharat Kolke MD (Med) - Physician - Criticare Asia Hosp. - Mumbai
Dr Mihir Raut - MD - Diabetologist - Nanavati Max Hosp - Mumbai
Dr R K Singh MD DM (Interventional Cardiologist) - Gandhi Medical College - Bhopal
frontiersin.org/journals/nutri…