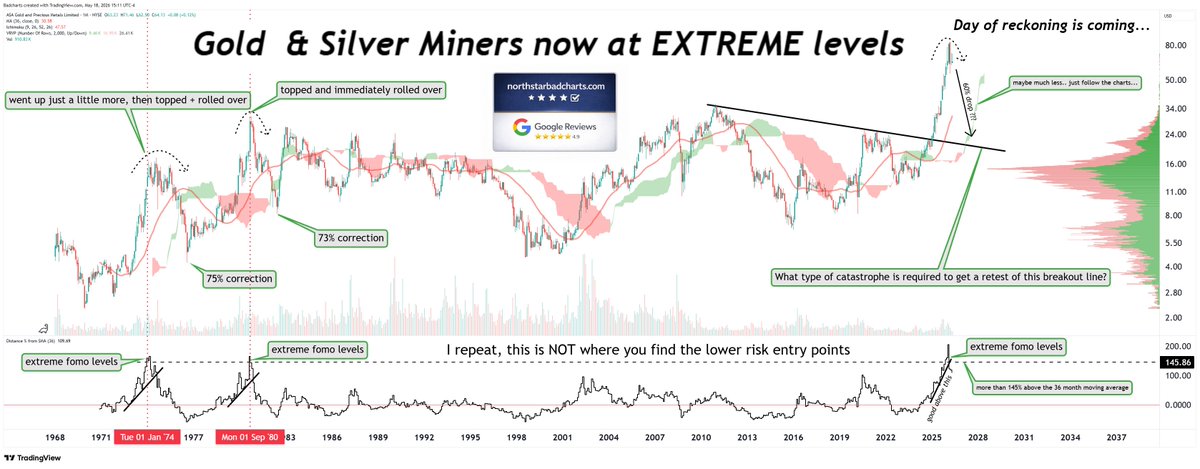
@DonDurrett @badcharts1 Wrong chart to post in response. Patrick’s chart covers a miner, yours is a chart of relative strength (gold v S&P). Not apples to apples. Gold could actually drop in price but rise on your chart if the S&P drops by a greater % within a similar timeframe.
English