@usamasyedMD Haven't heard of a bigger crap story today than this. Examination is absolutely essential in neurology and I'm sure in other specialties as well
English
Dr. Farhan Ansari, MD. DM
100 posts
@docfarhan88
Parkinson's Disease and Movement Disorders Specialist Consultant Neurologist

Has anyone else noticed doctors not….examining them anymore?





I’ll never really understand the craze around MD/MS (at least MD). DNB offers a far better work–life balance, along with stronger hands-on exposure in medical branches, and access to better diagnostic equipment for managing cases. Still underrated, somehow. #medtwitter #neetpg
Low back pain has the highest global prevalence of all musculoskeletal conditions. A new Video in Clinical Medicine demonstrates how to perform a physical examination of the lumbar spine. Watch the full video and read the accompanying article: nejm.org/doi/full/10.10…
Case discussion for doctors: Migraine aura or TIA? History A 48-year-old man presented with: 🔸Sudden visual obscuration involving right hemifield. This lasted for 15–20 minutes, followed by complete recovery 🔸This was followed by severe headache (7–8 hours) Workup elsewhere (by a senior neurologist): 🔸MRI: tiny right corona radiata FLAIR hyperintensity 🔸MRA, carotid Doppler: normal 🔸No DM/HTN/dyslipidemia 🔸Mild OSA (on polysomnography), insulin resistance (raised HOMA IR) ▶️He was diagnosed as “Old lacunar infarct + TIA (amaurosis fugax), and was started on aspirin + statin. This was more than a year ago. He consulted me for a second opinion. ❓Do you agree with the diagnosis? ❓Can it be migraine with visual aura?









🚨 SURGEON’S CAREER IS OVER after she got caught DANCING and TWIRLING a scalpel while patients were UNDER ANESTHESIA! One victim now has permanent, debilitating BRAIN DAMAGE. Videos show her rapping and acting like a total clown in the OR.





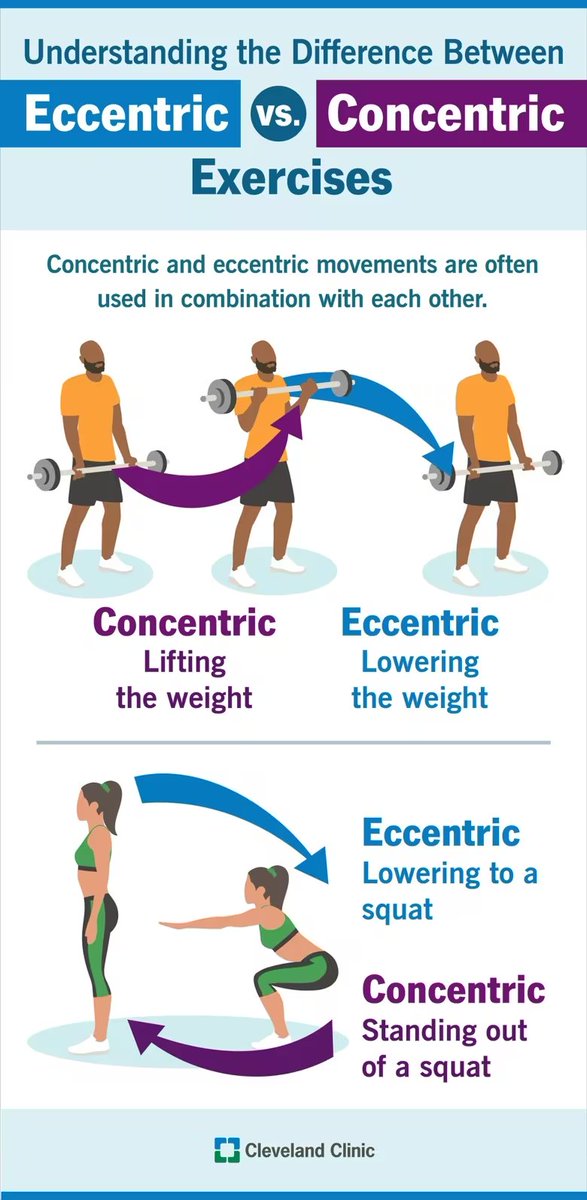
Deadlifts aren’t intrinsically dangerous. DON’T lift too heavy if you’re worried about injuries, that’s all. I slightly bend my knees so that tension is also on my hamstrings.
Teaching Video for junior doctors Analyze the gait of this 60-year old man; also observe his hands. He has had these symptoms for the past one year. He has no clinical evidence of supranuclear gaze palsy or backward falls. He also has no bladder or bowel symptoms. 1. Describe your findings. 2. What is the likely diagnosis? #medtwitter #neurotwitter