Dr Thomas Keeble retweetledi

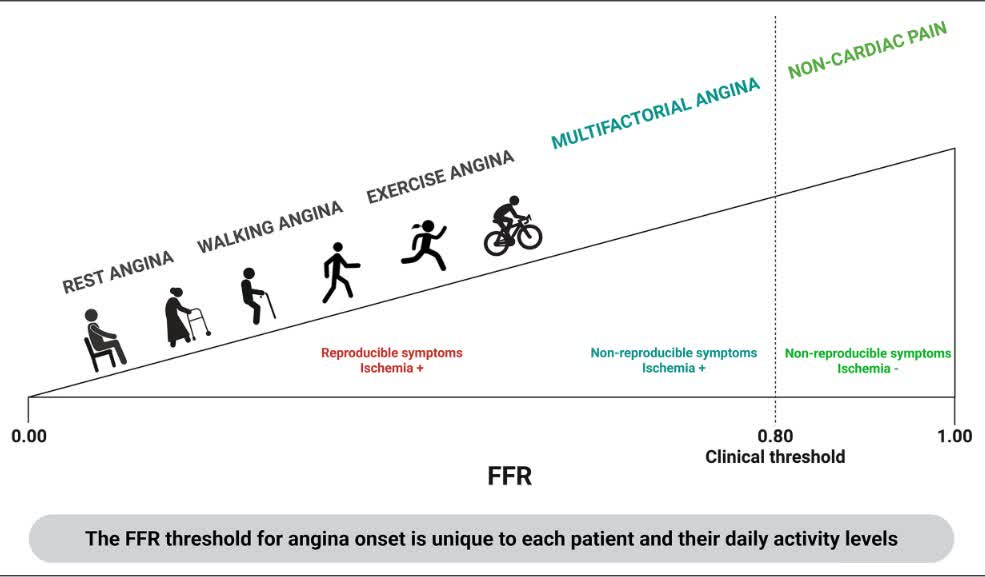
ORBITA-FIRE suggests universal Ischemia-based thresholds for FFR and non-hyperemic pressure ratio should be interpreted with caution: Integrating symptom-linked physiology may refine PCI selection and improve symptomatic response.ahajrnls.org/3R6AzQD
English