Dr. Ambily K retweetledi

🚨 Resistant Hypertension: From “Apparent” to “True” — Precision Matters (JAMA 2026)
🔬 Definition & Epidemiology — Not All Resistant HTN is Real
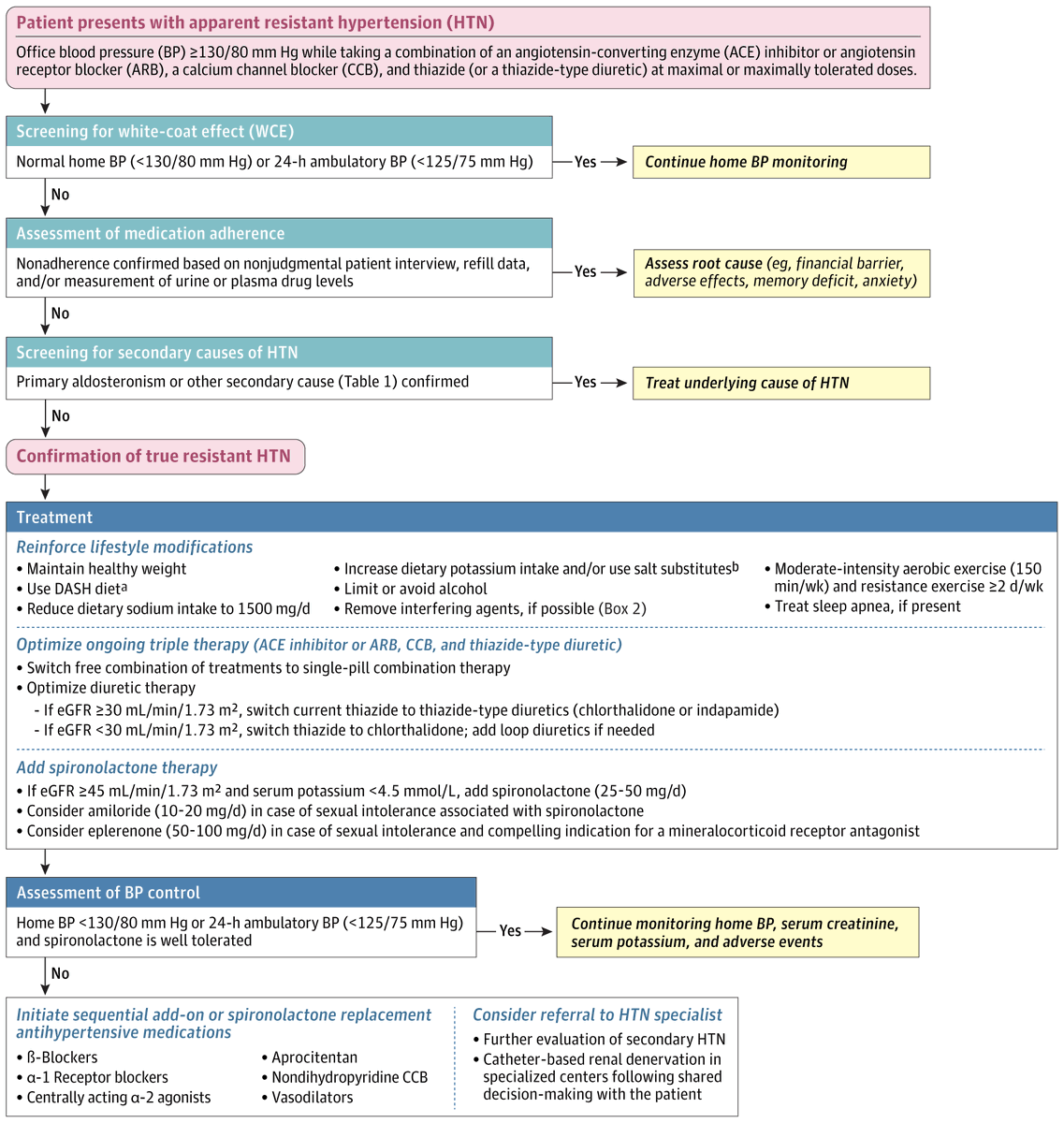
Apparent resistant HTN = BP ≥130/80 mm Hg despite ≥3 drugs (ACEi/ARB + CCB + thiazide) at optimal doses
~20% of treated hypertensives fall into this category
BUT → True resistant HTN ≈10% only after exclusion of:
White-coat effect (~37.5%)
Nonadherence (~50%)
Secondary causes (~5–25%)
👉 Clinical message: Most “resistant HTN” is pseudo-resistant → diagnosis refinement is critical
🧠 Stepwise Diagnostic Algorithm (High-Yield Clinical Thinking)
1️⃣ Exclude White-Coat Effect
Home BP <130/80 OR ABPM <125/75 mm Hg
➡️ Continue monitoring, no overtreatment
2️⃣ Assess Adherence (Underrated Step)
Use refill data / drug assays
Address:
Cost barriers
Adverse effects
Cognitive issues
3️⃣ Screen Secondary Causes
Primary aldosteronism (commonest)
CKD, OSA, obesity, drugs (NSAIDs, SNRIs, cocaine)
👉 Only after this → TRUE resistant HTN confirmed
⚠️ Why It Matters (Prognostic Impact)
↑ Cardiovascular mortality risk (absolute ↑ ~10% over 5–10 yrs)
Strong association with:
Diabetes
CKD
Obesity
Sleep apnea
🧬 Therapeutic Strategy — CME India Algorithmic Pearls
🔹 Step 1: Lifestyle (Foundation Therapy)
Sodium <1500 mg/day
Weight loss + exercise ≥150 min/week
Avoid alcohol, offending drugs
Treat OSA
👉 Often neglected but high-yield in India
🔹 Step 2: Optimize Triple Therapy
Prefer single-pill combinations (↑ adherence, ↓ SBP ~4 mmHg)
Diuretic optimization:
Chlorthalidone > thiazide (especially CKD)
Add loop diuretic if eGFR <30
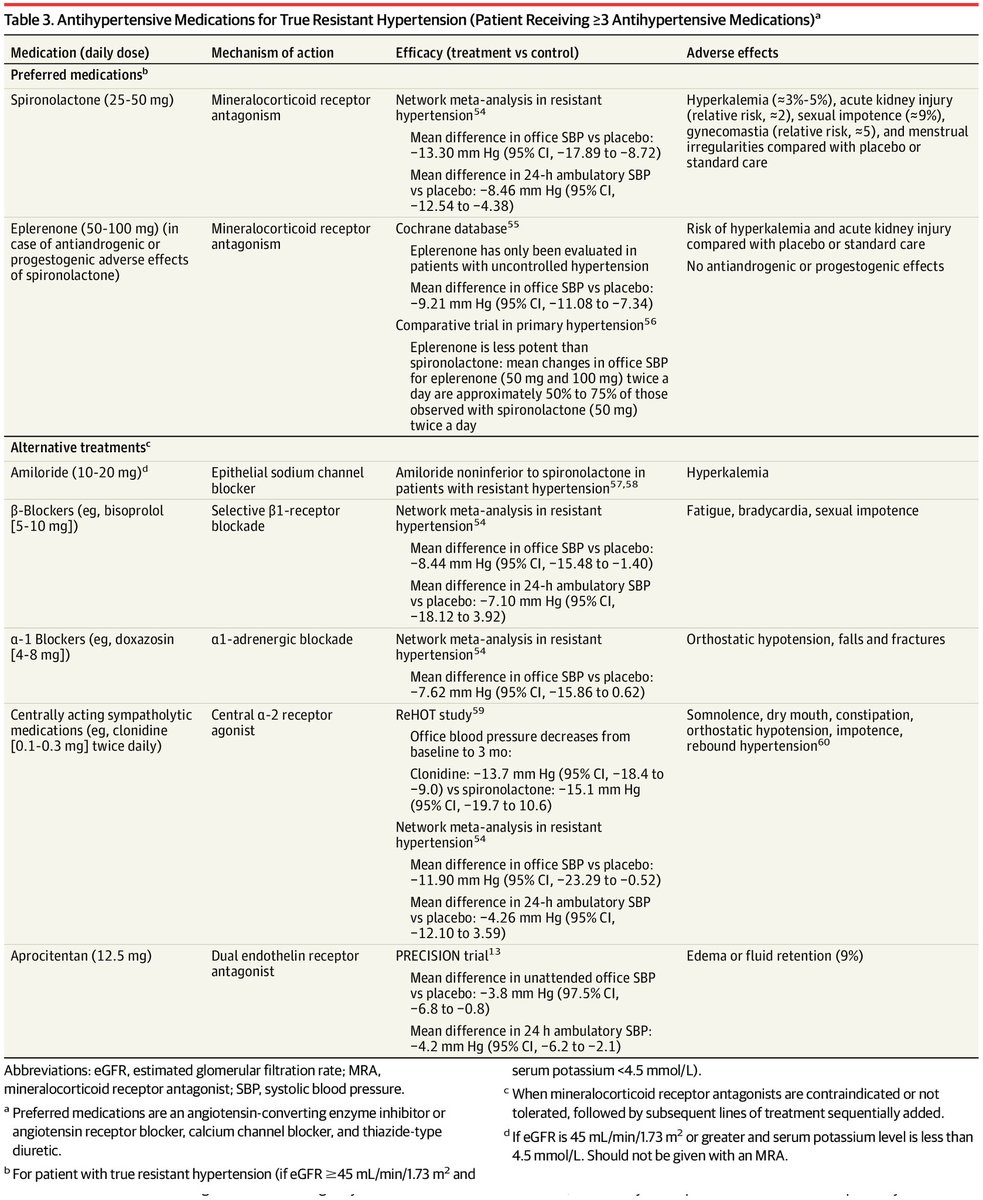
🔹 Step 3: Add Mineralocorticoid Receptor Antagonist (MRA) — ⭐ GAME CHANGER
Spironolactone 25–50 mg/day
↓ Office SBP: ~13 mmHg
↓ Ambulatory SBP: ~8 mmHg
Criteria:
eGFR ≥45 ml/min
K⁺ ≤4.5 mmol/L
👉 Most effective add-on therapy in resistant HTN
🔹 If Spironolactone Intolerance
Amiloride (non-inferior)
Eplerenone (less potent, fewer endocrine effects)
🔹 Step 4: Sequential Add-ons
β-blockers
α1-blockers (doxazosin)
Central agents (clonidine)
Non-DHP CCB
Vasodilators
Aprocitentan (dual endothelin antagonist — emerging option)
🔹 Step 5: Device Therapy
Renal denervation
↓ Ambulatory SBP ~4.4 mmHg
↓ Office SBP ~6.6 mmHg
👉 For selected refractory cases
💊 Drug Hierarchy (Practical Take-Home)
👉 Best Add-On:
✔️ Spironolactone > all others
👉 Alternatives:
✔️ Amiloride ≈ spironolactone
✔️ Eplerenone (safer endocrine profile)
👉 Less Effective / Add-on:
β-blockers, α-blockers, clonidine
👉 New Kid:
Aprocitentan (modest effect, fluid retention risk)
⚠️ Adverse Effect Awareness
Spironolactone:
Hyperkalemia (3–5%)
Gynecomastia (~5–9%)
Clonidine:
Rebound HTN
α-blockers:
Orthostatic hypotension
🎯 CME INDIA CLINICAL PEARLS
🔴 “Resistant HTN is often diagnostic failure, not therapeutic failure”
🔴 “Half of resistant HTN = nonadherence → always check before escalating”
🔴 “Chlorthalidone + Spironolactone = backbone of resistant HTN therapy”
🔴 “Primary aldosteronism is underdiagnosed → think beyond essential HTN”
🔴 “Single-pill combinations are not convenience—they are outcome modifiers”
🔴 “Renal denervation: modest BP fall but useful in selected refractory cases”
📚 Key Reference (Journal Format)
Carey RM, et al. Resistant Hypertension: Diagnosis and Management. JAMA. 2026; doi:10.1001/jama.2026.2846682
jamanetwork.com/journals/jama/…
English