Sabitlenmiş Tweet

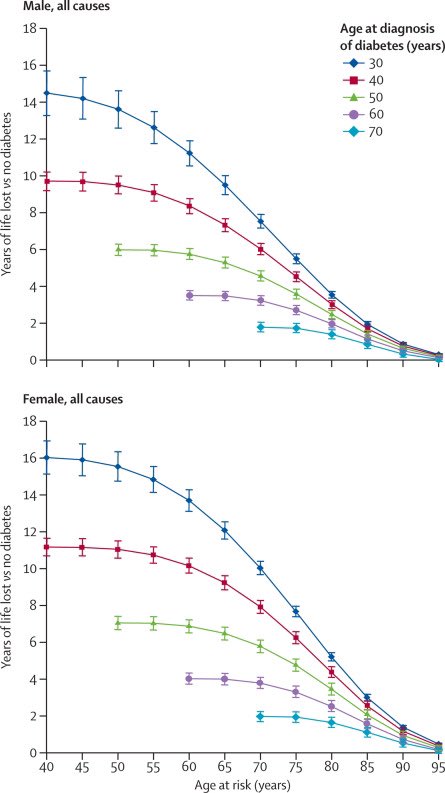
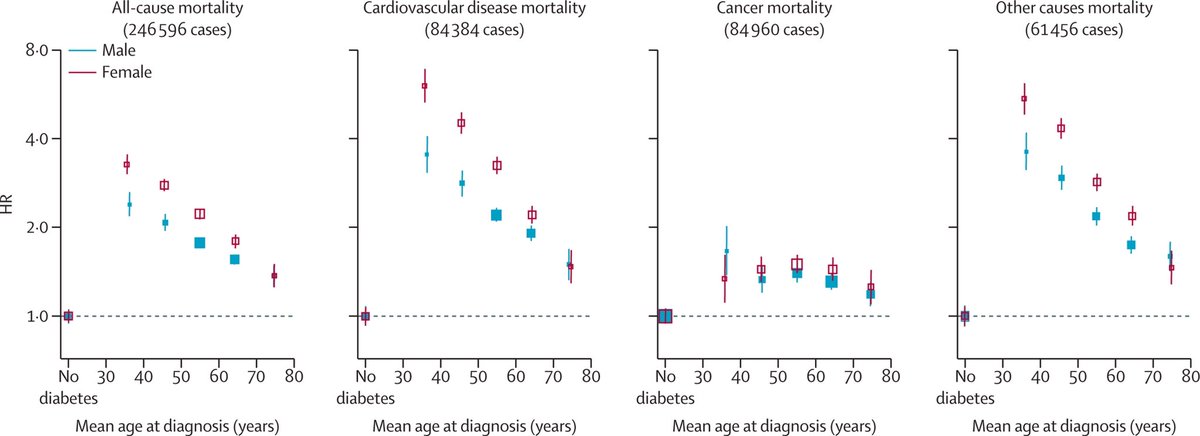
📍Life expectancy ⤵️ by 3-4y for each decade diagnosis of #type2diabetes before 70y
📍driven by ⤴️ CV ☠️
👉 important to manage all, but the #T2Day cohort especially need our attention
@ShivaniM_KC
@kamleshkhunti @Dralbalawi1989
thelancet.com/journals/landi…
English