Sabitlenmiş Tweet

Rajat Goyal
1.3K posts

@drrgoyal
Cardiac Electrophysiologist @Sutterhealth - California Pacific Medical Center. Dad Joke Expert. Views are my own.


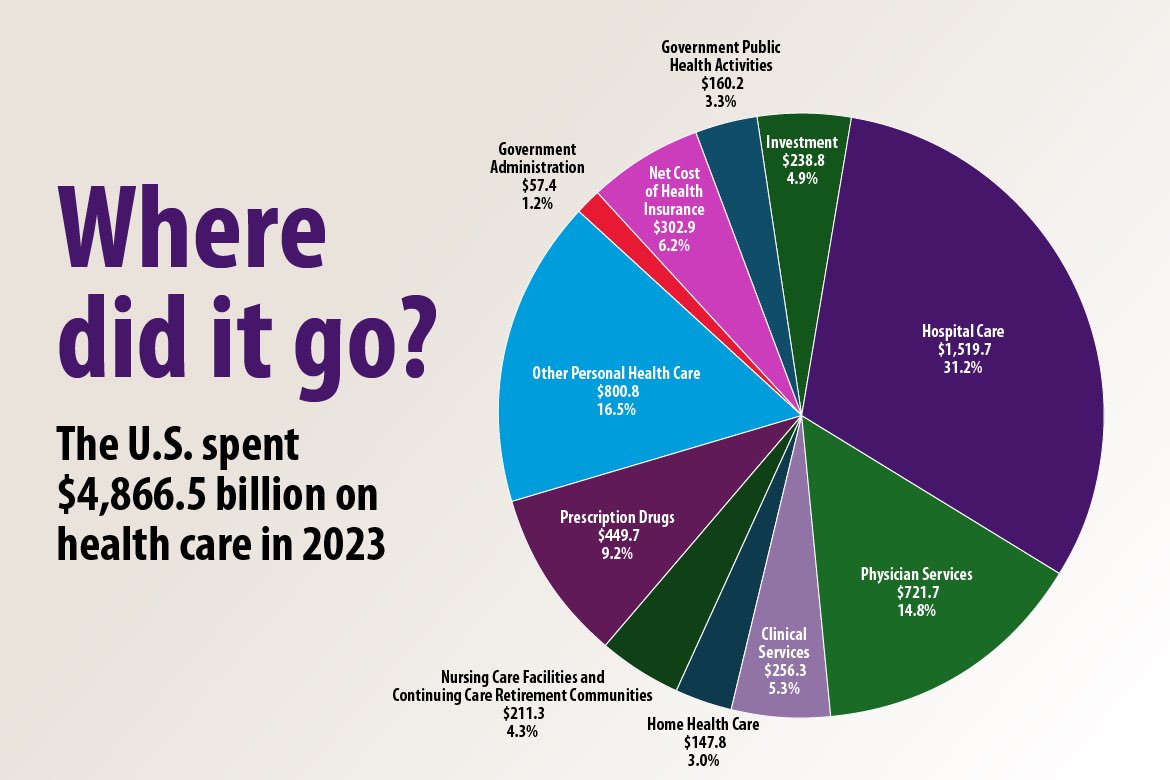
@SpineNeuro This is only part of the payment... a small part. Does not include the hospital. Total costs are $30-50K or more. Let's have a real discussion rather than clickbait.















And the debate continues PhysioSync trial ⬇️⬇️⬇️ CSP is inferior to BiVP for CRT in HFrEF and LBBB (QRSD ≥ 130 msec) including HF events, LVEF improvement and death #EPeeps #ESCCongress

Ditto that for spine surgery. Never seen this level of friction for approvals that would have been routine not even 24 months ago. The latest tactic - need to specify the vendor for any spine implants as well as the corresponding CPT code. Any mismatch? They get to deny solely on that basis. Have multiple patients who had their surgeries approved, but not the spinal implant. That would require - you guessed it - another peer to peer query and probably a formal appeal. Also never had to send so many people for direct hospital admission w progressive neurologic deficits because of delays w these insurance approvals. (Literal bladder incontinence and weak leg where our pre cert folks spent 17 HOURS trying to navigate the approvals process and they still denied surgery.) 4 years of med school 8 years of post graduate clinical training 24 years in clinical practice Yet I am still at the mercy of a consolidated financial bureaucracy run by an accounting major/MBA from Snickerdoodle University who managed to pledge the right fraternity and played golf w the third cousin of someone who knew Paul Tsongas' grandkids barber.

American Physician Assistant who has worked in cardiology for 8 years says “I have NEVER seen so many echos denied like I have this year” She says health insurance companies are denying routine scans at rates like never before and making it harder to appeal. Just this one phone call she spent 41 minutes of her lunch trying to get approved through the prior authorization department This video shows how many runarounds and multiple numbers and transfers the insurance companies make doctors offices go through, making it literally impossible to get things approved Health insurance companies just keep getting worse and worse