Eleonora Teplinsky, MD, FASCO retweetledi

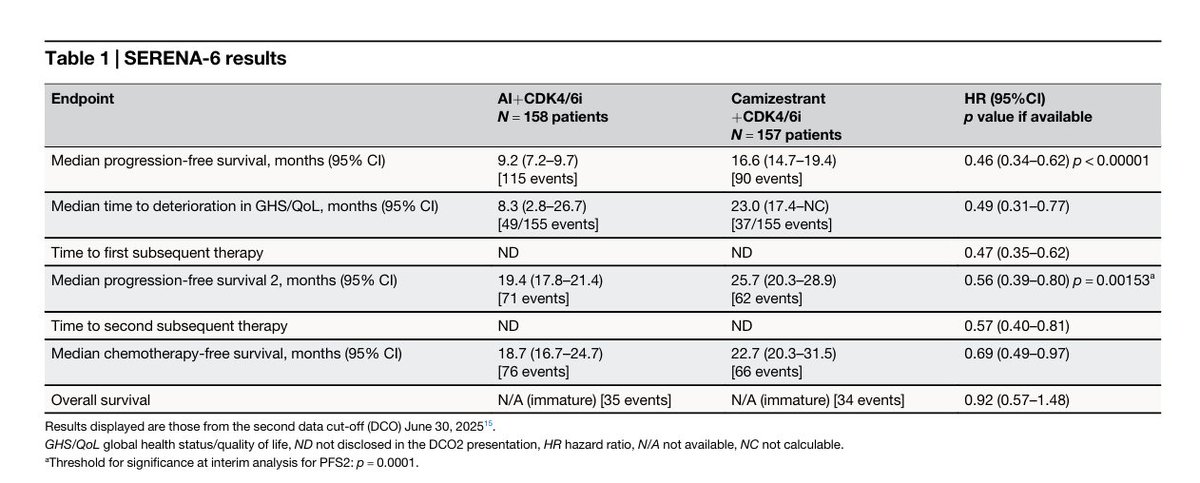
Letter in @Nature_NPJ👉SERENA-6 interpretation and clinical implications: intercepting endocrine resistance in #MetastaticBreastCancer.
🔓pubmed.ncbi.nlm.nih.gov/42259831/
@BianchiniGP @breastoncdoc @JavierCortesMD @curijoey @Shaheenah1 @LGerratana @antgiorda @MIgnatiadis @KalinskyKevin @elmayermd @BCJoyceO @drsarahsam @PedramRazaviMD @PTarantinoMD @GustavoWerutsky #MBC


English