Sabitlenmiş Tweet

Please subscribe my YouTube channel: bit.ly/2DWogkJ
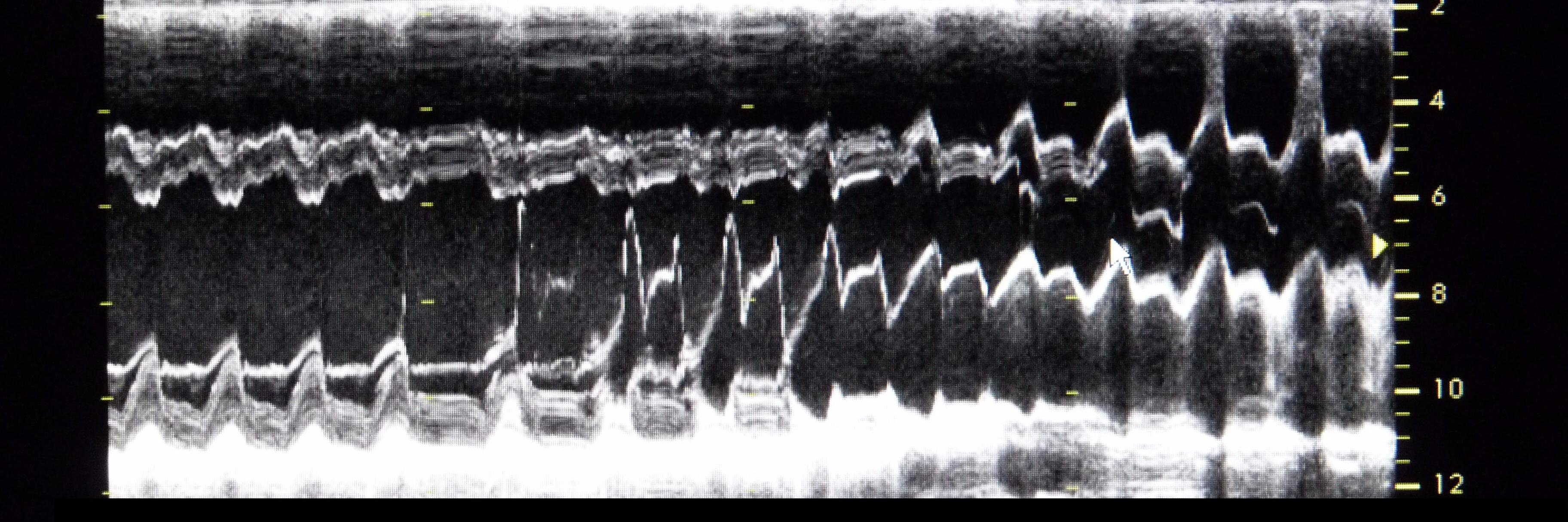
I would like to present my project (echocardiography step by step®). With my project, I want to take you into the world of echocardiography through the prism of my experience.
English