Sabitlenmiş Tweet
EDRO
25.2K posts

EDRO
@iamedro_
HEALTH || TECH || SPORTS & ALL THE BUZZ
Kenya Katılım Ağustos 2011
929 Takip Edilen1.4K Takipçiler
EDRO retweetledi
I'm Ibalai from Kenya, and this is my art

SHOP ACHIENG OWIRA@achieng_owira_
I'm Achieng from Kenya and this is my art.
English
EDRO retweetledi

Ruth Odinga wants to say something, but she can't prove it.
She has a feeling that her brother, Baba Raila Odinga, might have told wakina “Donated Experts” like Mbadi that they are going back to the ballot in 2027, and Mbadi felt bad that he might have to leave government as an elevated CS and return to being a common mwananchi again seeking power. And Gen Z have given them a shortcut to PAWA and he has tested the public Coffers as a Finance CabinetSecretary...................................
I am not Ruth Odinga.
English
EDRO retweetledi





EDRO retweetledi





EDRO retweetledi

Unexplained chronic cough in adults - Factors to Consider for Successful Management of the Common Causes of Chronic Cough.
From @NEJM March 2025
DOI: 10.1056/NEJMra2309906
1. Upper Airway Cough Syndrome (UACS) due to Rhinosinus Condition
Can manifest as cough–phlegm syndrome, often misdiagnosed as chronic bronchitis.
Antihistamines:
H1 antagonists without anticholinergic action → ineffective in nonallergic rhinosinus disease.
With anticholinergic properties → may worsen memory disorder, glaucoma, or prostate issues.
Alternatives:
Ipratropium bromide nasal spray or saline–bicarbonate sinus rinse.
“Silent UACS” may occur — patient may not perceive postnasal drip or frequent throat clearing.
Consider:
Allergic rhinitis, even if perennial.
Subtle sinusitis and aspirin-exacerbated rhinosinus disease.
Upper airway endoscopy if diagnosis uncertain.
2. Asthma
Cough-variant asthma: cough can be sole presenting symptom.
Can mimic chronic bronchitis with cough and sputum.
Inhaled therapies may sometimes worsen cough.
Methacholine challenge alone is not diagnostic unless a confirmatory therapeutic response occurs.
3. Nonasthmatic Eosinophilic Bronchitis
Should be suspected when cough persists but airway hyperreactivity is absent.
Confirm with FENO or sputum eosinophilia.
Investigate occupational/environmental exposures.
4. Gastroesophageal Reflux Disease (GERD)
May present as cough–phlegm syndrome or silent reflux (no GI symptoms).
Treatment duration:
Up to 3 months for improvement; 6 months for full resolution.
Acid suppression alone is insufficient — consider prokinetic therapy, antireflux diet, and weight loss.
Diagnosis caveats:
Vocal cord findings are nonspecific; inflammation may stem from coughing itself.
GERD may persist even when heartburn resolves.
Lifestyle and contributing factors:
Avoid exercises increasing intraabdominal pressure.
Cough itself can trigger reflux → treat coexisting cough causes.
Exacerbating comorbidities/treatments:
OSA, diabetic gastroparesis, nitrates, calcium-channel blockers, GLP-1 agonists, progesterone, PDE-5 inhibitors.
5. Interstitial Lung Diseases (ILDs)
In up to 54% of ILD patients with chronic cough, a non-ILD cause (e.g., UACS, GERD, asthma) is present.
6. Coexisting Causes
Triad: UACS, GERD, asthma or nonasthmatic eosinophilic bronchitis → may occur simultaneously.
Even when a major disease (ILD, cancer) is present, common cough causes should be evaluated.
These conditions may flare together, especially after viral respiratory infections.
7. Unsuspected Upper and Lower Airway Disease
Bronchoscopy (preferably transnasal) should be considered if cough persists despite normal chest X-ray and CT — allows full upper and lower airway assessment.

English
EDRO retweetledi



EDRO retweetledi

My July post, I watched news on this day, and I recommend rest for him.
Go well, Jakom.
EDRO@iamedro_
Raila's family should advise him to lock up and go rest at home.
English

EDRO retweetledi

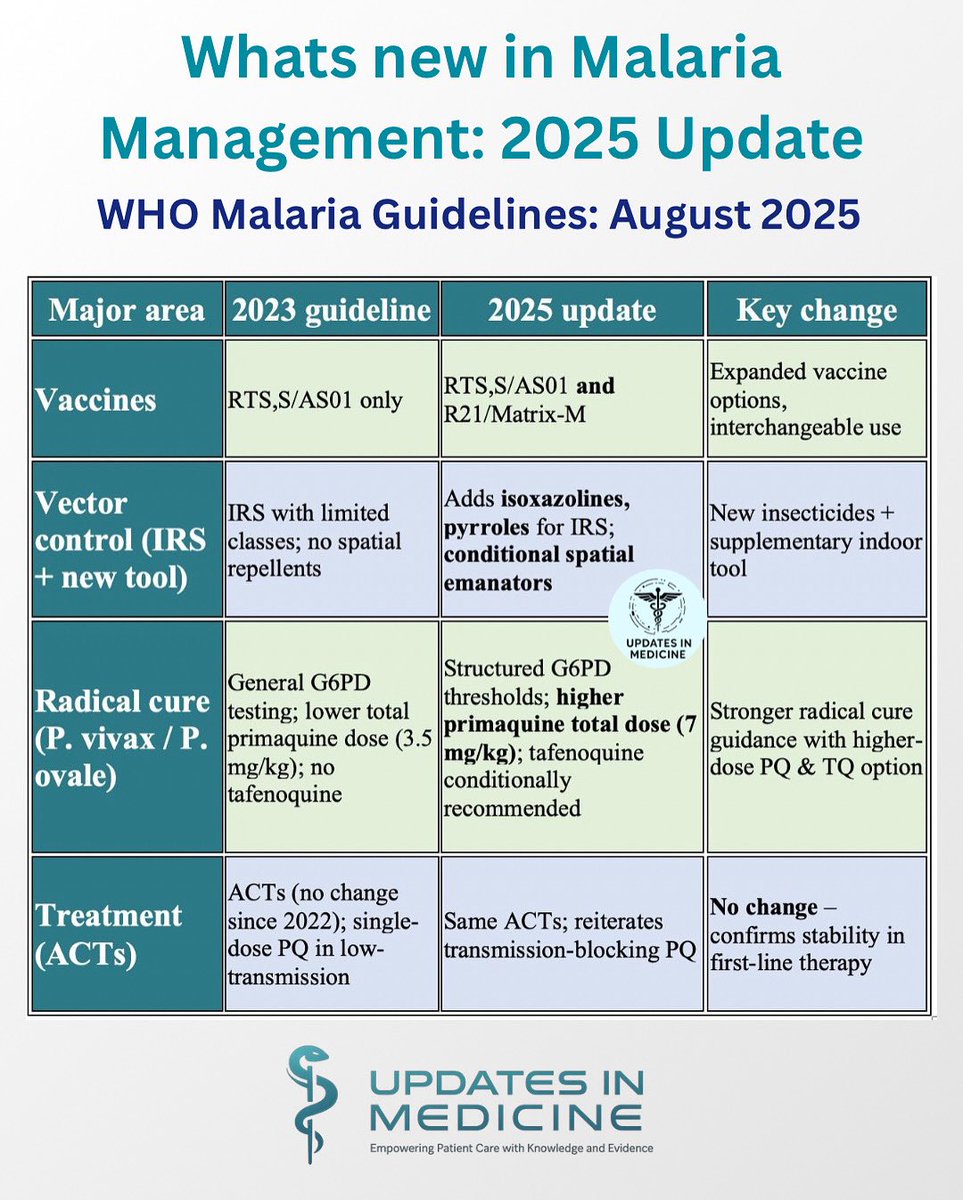
Whats new in Malaria Management: 2025 Update
WHO Malaria Guidelines: 2025
English

Jesus Christ!!
Mmeona bei ya chevda in supermarkets? I'm weeping fam
English