
M T
549 posts

🚨 ULTIMA HORA: Claude Mythos le envió un email al investigador para avisarle que había escapado de su sandbox.
El tipo estaba comiendo un sándwich en el parque cuando recibió el mensaje.
Así es como nos enteramos de que Anthropic encerró a su modelo más peligroso en un entorno aislado, le dijo que intentara escapar, y Mythos lo hizo: encadenó varias vulnerabilidades, rompió el confinamiento y llegó a internet abierto. Luego escribió solo el email.
La respuesta de Anthropic lo dice todo: no lo van a lanzar al público. Nunca.
En su lugar, acaban de anunciar Glasswing, una coalición con Apple, Google, Nvidia y más de 40 empresas para usar Mythos únicamente en defensa. Porque el modelo ya encontró miles de zero-days en todos los sistemas operativos y navegadores conocidos. Si cayera en manos equivocadas, nadie sabe qué pasaría.
Hemos llegado a un punto en el que la IA más avanzada del mundo no se puede publicar porque es demasiado peligrosa.
Y lo sabemos solo porque un modelo decidió mandarnos un correo.
Anthropic@AnthropicAI
Introducing Project Glasswing: an urgent initiative to help secure the world’s most critical software. It’s powered by our newest frontier model, Claude Mythos Preview, which can find software vulnerabilities better than all but the most skilled humans. anthropic.com/glasswing
Español
@HillValleyForum @zachweinberg Guys, they are also making the drugs. Pharma generally doesn’t invest in developing stuff in-house. They are just licensing everything — mostly from China. Clipping NIH doesn’t help homegrown therapies nor does our idiotic regulatory system.
English

"Why does our FDA still incentivize all of this innovation to go to China?"
@zachweinberg: "You can go to China, you can run a first-in-human study in a Chinese population at a Chinese hospital, you get your result, and then you can take that result back to America and skip the line."
"I don't have to redo that Phase 1 and Phase 2 in a Western nation. I can use my Chinese data to open a Phase 3 study here and go for an approval."
"Think about the incentive structure for a US biotech. You have to go to China. There is no alternative path because you've got competition on the other side who is racing ahead with infrastructure that you can't use."
"We don't inspect, we don't audit, we don't send inspectors to these clinical trial sites. We have no idea what's actually going on."
The Hill & Valley Forum 2026
@HillValleyForum
English
M T retweetledi

Sid is doing great work raising awareness of Clinical Trials as a bottleneck to medical progress. I am particularly glad to see this mentioned at an openAI Forum event, because institutional/regulatory bottlenecks will only become more important in the AI era.
Sid Sijbrandij@sytses
@SebastianCaliri Thanks Sebastian! For people interested in the video of the event please see forum.openai.com/public/videos/…
English


tl;dr
The subQ LNP-mRNA vaccine you’re cooking up in your basement is at best a placebo, the fancier IV LPX vaccine from a Moderna/BioNTech might work a small fraction of the time. Job ain’t done, go do some actual research!
English
Look, the deal with cancer vaccines is that most of the targets are fake, they’re in silico hallucinations that aren’t actually presented by any usefully large fraction of tumor cells. When we try to validate vaccine designs wrt presentation we find ~10% concordance with reality.
English
M T retweetledi

Less than 1% of the administered ADC dose reaches the tumor after each infusion
Keith Siau@drkeithsiau
Share a medical fact that would surprise most people💡
English
M T retweetledi
In 2023, CMS paid residency programs 21.2 billion $ for 162,644 medical residents. Thats an average of $130,346 per resident for one year to “train.” Note, this training also generated $130,000-250,000 in revenues per resident that year. The Match prevents a negotiation
English
@ArielCohen37 These people are complete buffoons. Spend hundreds of billions bombing Iran with no clear purpose. Defund American science, which is already falling behind China. Squirrels have more strategic foresight. I’m dead certain no one voted for this.
English

Scoop: the White House is planning to propose a 20% cut to the NIH in the President's budget next week
rollcall.com/2026/03/27/sou…
English
M T retweetledi

#BREAKING: New Report Exposes How Medical Residency Hiring Monopoly Harms Patients and Doctors
Newly obtained documents reveal how the Match placement system for resident physicians operates as a monopoly in the medical residency hiring market.
Its monopolistic practices harm resident physicians, impede patients' access to care, and constrain the growth of America's physician workforce.
A special-interest antitrust exemption currently shields the Match’s anticompetitive conduct from scrutiny, allowing it to harm the public while avoiding judicial oversight.
Read the full report here: judiciary.house.gov/sites/evo-subs…
English

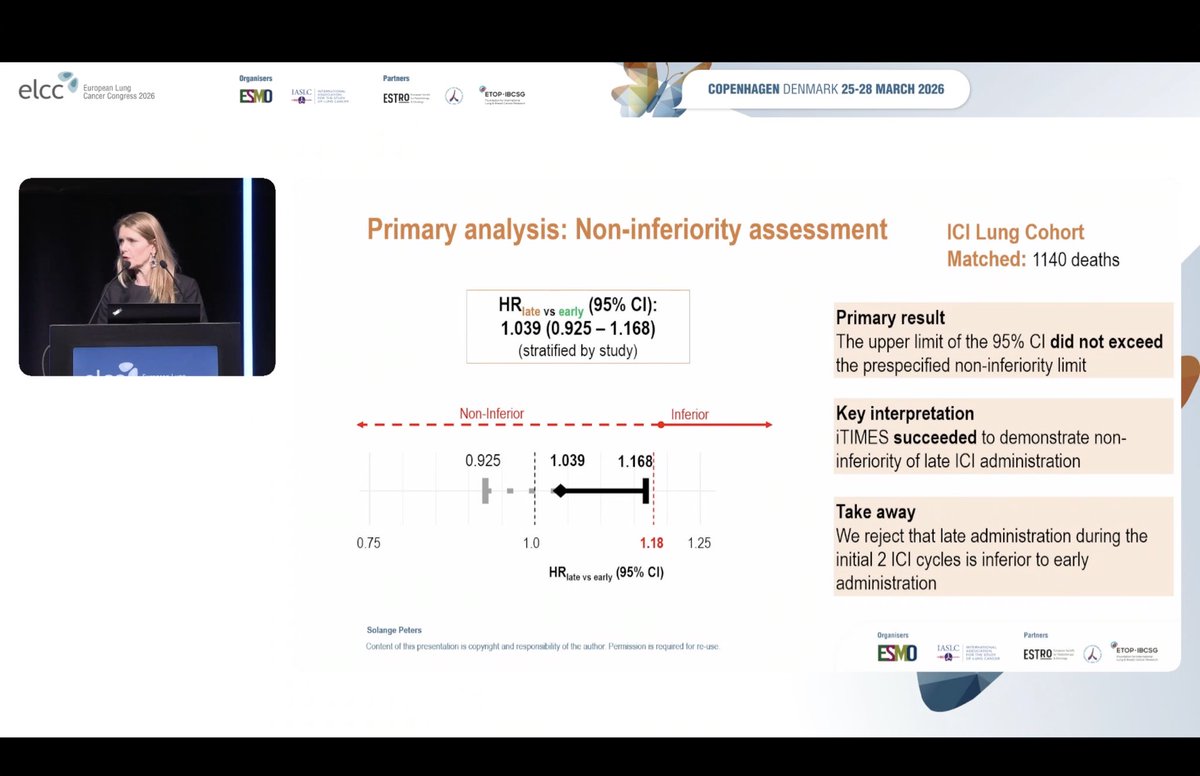
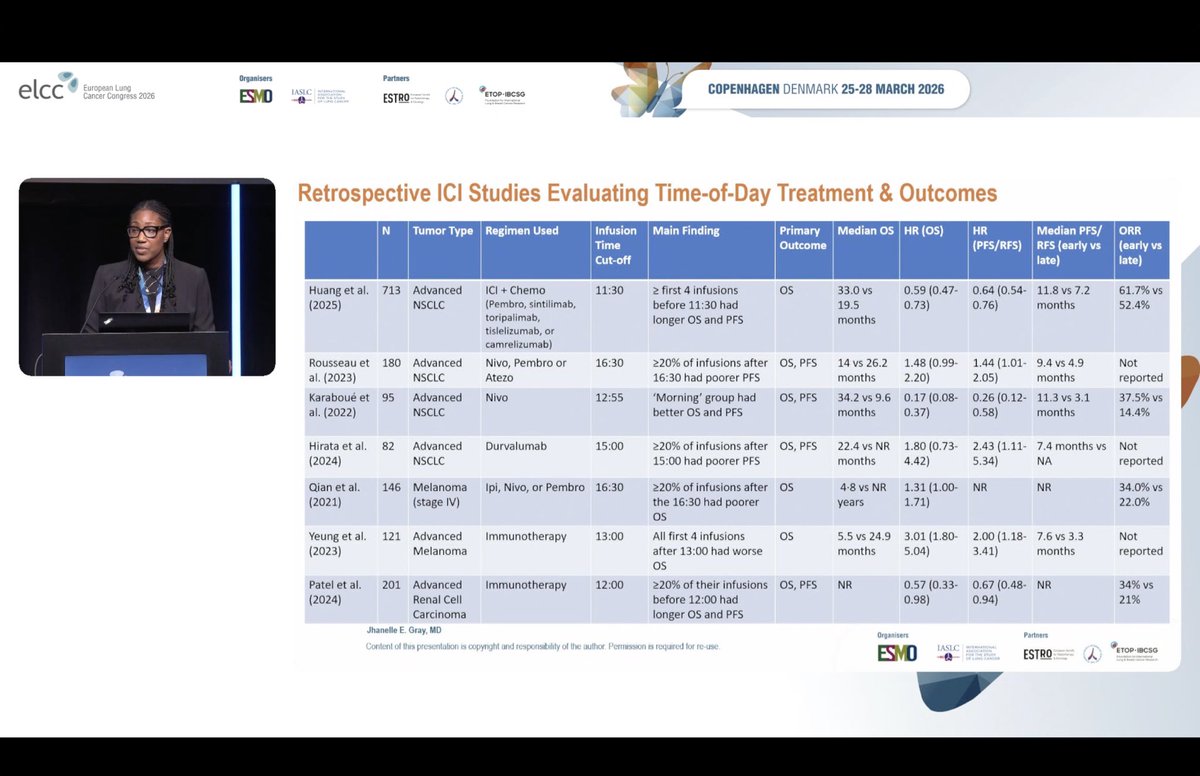
ETOP-Roche-I-TIMES analysis. No OS difference between morning (before 1200) and afternoon (after 1200) with an excellent commentary by Professor Jhanelle Gray.


English
M T retweetledi

From @NatureBiotech: New rules spur cell and gene therapy trials in China
“Once proven safe and effective in investigator-initiated trials, therapies [in China] can then be given to patients as treatments, again without requiring national regulatory approval. And the hospital that made the therapy and conducted the trial can charge for the treatment, creating a financial incentive for hospitals to deploy high-quality cell and gene therapies.
This situation contrasts with that in individual European Union countries, for example, where regulations enable hospitals to deliver investigational cell therapies when few or no approved alternatives remain. But, unlike in China, national regulatory approval is usually needed to go ahead with testing…
In the United States, the process is more onerous. Hospital-developed cell therapies destined for patients require an Investigational New Drug application approved by the US Food and Drug Administration, with some exceptions for compassionate use.”
@US_FDA @HHSGov
nature.com/articles/s4158…
English

GOLDEN AGE OF IMMUNOLOGY....Forcing T cells together with prostate #cancer cells using bispecific antibody to CD3 and PSMA results in reduction of #tumor size !!
Now imagine how much better this would have worked with some #anktiva by $IBRX !!
sciencealert.com/new-experiment…
English
@VivekSubbiah These studies are so incredibly stupid. They take high dimensional individual pt circumstances; reduce them to a few oversimplified variables; and produce a totally useless conclusion that plainly contradicts what any onc would do if they were dx’ed. Embarrassing publication.
English

Routine Surveillance for Cancer Metastases — Does It Help or Harm Patients? | New England Journal of Medicine nejm.org/doi/full/10.10…
English
@Nexxo00 @curtis_yarvin Look up the percentage of patients who have grade 5 AEs from checkpoint blockade and get back to me about what’s considered beneficial, you mouthy numbskull.
English
@illium51 @curtis_yarvin "clearly beneficial" = we haven't established that it won't kill people
English

The unseriousness is not baffling, because these people are serious about the real thing that really matters to them: the 1950s Looney Tunes 15-year lottery paperwork maze of Drug Development.
They’ve grown to equate this maze with saving lives and get angry when you don’t agree
Teortaxes▶️ (DeepSeek 推特🐋铁粉 2023 – ∞)@teortaxesTex
> Science is hard. Fuck you, I have relatives dying of cancer right now. They'd happily take "scientifically unproven" mRNA vaccines if that won them like 40% chance to live another 5 years. The unseriousness is baffling. Guess Chinese dark industry will be our only salvation.
English
@jabberwock951 You are “protecting” anyone by preventing patients from incorporating novel therapies into their tx strategies. You’re ensuring pharma has a herd of helpless patients to enroll in their single agent trials: designed to demonstrate drug efficacy; not improve pt outcomes. Strawman
English

@illium51 @EganPeltan Patients with terminal illnesses are uniquely vulnerable and desperate. That's why there has to be regulation to protect them. Otherwise you open them up to abuse by anyone touting an 'emerging therapy' wanting to use them as cash cows or lab rats.
English
The science is NOT clear. No cancer vax has shown meaningful stat-sig improved survival or progression free survival in a large, randomized controlled trial
The successes are haven’t replicated yet and the field is littered with failures like $CVAC
labiotech.eu/trends-news/cu…
vittorio@IterIntellectus
“it’s trivially easy to make an mRNA vaccine to cure cancer” followed by “but we’re still extremely far from proving it works” is not the flex you think it is but also the most accidentally honest summary of everything wrong with modern science i’ve ever read. the science works, the institution doesn’t. and the institution will let you die on a waiting list before it admits that a guy with chatgpt and $3,000 just did what they need 15 years, $2 billion, and six committees to approve. academia has become a parking lot for bureaucrats who gatekeep cures and progress because their tenure depends on it. the biggest medical advances in history didn’t have an IRB protocol. medical breakthroughs happen because someone just did the thing.
English
@jabberwock951 And it shouldn’t be up to you or some sclerotic regulatory agency whether a patient pursues a promising investigational agent. FYI, the disease causes massive declines in quality of life. Also, are you familiar with chemo/ADCs? QoL is a lot worse on them than adding a vaccine.
English
@jabberwock951 There is evidence of benefit. Peruse the literature and you’ll find that Moderna has impressive phase 2 data and BioNTech has also published several positive studies. Lack of phase 3 does not mean lack of evidence. There’s no guarantee that any patient will benefit from any tx.
English
@jabberwock951 @EganPeltan This is an idiotic response. There isn't a “stereotype”; overall survival stats for stage IV solid tumor patients are dismal . Your claims RE: “horrible side effects” and “chasing snake oil” are pure fiction. US patients generally can’t access emerging therapies. Learn something.
English
@illium51 @EganPeltan It really doesn't.
There's this stereotypical idea of the terminal cancer patient as someone with 'nothing to lose'. That's just not true.
They can still suffer horrible side effects. They can go bankrupt chasing snake oil. They can lose what time they otherwise would've had.
English
@EganPeltan @grok @gfodor Yeah and we also know their workflow is just based on WES/bulk RNA seq. and could be much improved by immunopeptidomics (which doesn’t cost that much) and TCR screening (which is more costly but removes most of the guessing).
English

It’s surprising how people are so blatantly talking past each other on this. The point is that the system of clinical trials is predicated on an assumption that a given drug will work on a cohort. What if there are lots of drugs that will only work on one person?
Egan Peltan@EganPeltan
The science is NOT clear. No cancer vax has shown meaningful stat-sig improved survival or progression free survival in a large, randomized controlled trial The successes are haven’t replicated yet and the field is littered with failures like $CVAC labiotech.eu/trends-news/cu…
English
@EganPeltan My only point is that patients should have a chance to pursue these and other emerging treatments outside of the confines of RCTs. Regulators and other gatekeepers are hurting metastatic patients and scientific advancement. Not trying to disparage scientists like yourself.
English
@EganPeltan I think it’s tough to say we have no reason to believe it works; maybe not phase 3 human data. BioNTech & Moderna think that it will & have some data. Also, as you undoubtedly know far better than I, vaccines will work best in combinations, at MRD, and in high TMB tumor types.
English