
David Krieser
533 posts
David Krieser
@kriesed
Paediatric Emergency Physician, Sometime educator, News junkie, Cavoodle owner
Mckinnon, Melbourne Katılım Haziran 2012
149 Takip Edilen347 Takipçiler

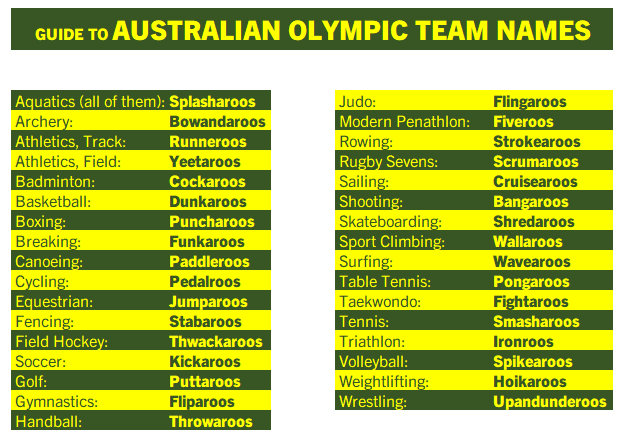
🇦🇺Australia is the only country whose #Olympics teams all have nicknames. As an honourary Australian, I thought I'd provide this handy guide for each so that you can cheer on your favorites:
English
David Krieser retweetledi

As a new Emergency Medicine attending 10 years ago I was asked to write about my insights into what it's like to be an ER Doctor. I just randomly came across it and after all these years I'm amazed by how much this all still rings true in my heart today. So I wanted to share it with you guys. Here's what I wrote:
MAKE THINGS HAPPEN, SAVE LIVES, ALLEVIATE SUFFERING
My Emergency Department is a battlefield. Volumes are high and the pace is fast. To succeed as an Emergency Physician I must be an expert of efficiency. I also must be an expert of triage. I am constantly triaging and re-triaging as things evolve. The ED is highly unpredictable. My entire shift I am on guard and ready for any emergency to come flying through the doors at any moment. In the meantime I am either taking care of or seeking out other emergencies. My job is not to be expert in all of medicine. My job is to be jack of all trades and master of diagnosing and treating what can and will kill you. If I cannot provide the definitive care you need, my job does not end until I have gotten you there.
The more I practice Emergency Medicine, the more I realize that what I do more than anything else is - make things happen. Cliff Reid (@cliffreid) delivered an excellent SMACC talk on making things happen in the resuscitation bay. (If you haven’t yet heard it I recommend you do). I’ve come to realize that this concept extends beyond the resus bay and pervades all aspects of my job.
So what does it mean to make things happen? Making things happen means putting my visions of what needs to happen into motion and making them reality.
In order to make things happen, I must first appreciate that my ED is equipped with an army of highly skilled staff that are the heart and soul of the department – and that without them I could make very little happen.
Making things happen means identifying a sick patient and getting them quickly moved to a critical bed; it means getting my suspected head bleed patient expeditiously to the CT scanner with least possible delay; it means mobilizing help to intervene on my flash pulmonary edema patient in hypertensive crisis and getting her on CPAP & Nitro immediately to pull her out of the water and prevent intubation; it means convincing my adamant patient who is ready to walk out the door but is clearly not well enough to go home not to sign out against medical advice, but rather to stay in the hospital where he/she is safe and taken care of; making things happen means advocating for my patients and convincing my consultants to take them emergently to the cath lab or operating room at 3 AM when it otherwise would not have happened until morning. Making things happen means constantly thinking two steps ahead. Making things happen is an art. I have learned that to excel in Emergency Medicine I must master the art of making things happen.
If my goal is to save lives, I must first recognize that a life needs to be saved – that is, I must be an expert at diagnosing life-threatening processes. The 75-year-old clutching his chest with tombstones on his ECG – that’s easy. The problem is that most of my patients are not truly sick. Some are here because they are afraid that they are sick, and just need reassurance. Some are here just for pain medications. Most of my patients are undifferentiated. Sickness is a spectrum. Truly sick patients often look sick, but often they do not. I must be expert at sifting through the crowd and identifying which patients are harboring a life-threatening diagnosis. This is not always an easy task, but it’s up to me to figure it out.
It’s my job to figure out that the 45-year-old gentleman who looks comfortable sitting up in bed watching television and texting on his phone has a Type A Aortic Dissection. If I simply get two sets of cardiac enzymes, repeat an ECG and discharge him home since these are normal – there is a good chance he will die. It’s my job to figure out that the 60-year-old lady with chest pain who was transferred to me for “NSTEMI” actually has a huge saddle pulmonary embolus. It’s not enough to just admit her to the hospital floor only for her to sit up there, decompensate, and have a bad outcome. I have to do better than that. In the Emergency Department, there are landmines scattered everywhere. It’s my job to find the landmines.
I can’t talk about saving lives without talking about Resuscitation. This is an entire topic in and of itself and I could write all day about it – but I won’t do that here. I will simply say that if I want to save lives, I must be an expert at Resuscitation. I believe that as an Emergency Physician, if I am not expert at Resuscitation – my purpose is lost and my mission is in vain. Resuscitation encapsulates those moments that matter most; the moments that often determine my patients’ fates, and define Emergency Medicine as a specialty. Resuscitation is the essence of Emergency Medicine.
In the end, Emergency Medicine is all about the patients. While patients are under my care, I consider them family. When I walk into a room, I shake hands with each patient and all their friends and family members who have come to support them. I look my patients in the eyes. I listen to them. I try my best to put myself in their shoes and empathize with them. I know that communication is vital and I make sure we are on the same page, and that all of their questions have been answered. I make a point to ensure that they know to let me know if they need anything. If my patients are not comfortable, I am not comfortable.
Some humble advice I have to offer for success in Emergency Medicine:
1. Never stop learning. There’s too much out there to know, and knowledge is the foundation for the care we provide. Your eyes won’t see what your mind doesn’t know. Never get complacent in your knowledge.
2. Trust your instincts. Gestalt is at the heart of what we do. Without it we are merely computers and robots. Gestalt trumps any clinical decision rule any day. Even if you don’t know exactly what’s wrong with your patient, but you have a feeling something bad is going on – trust it and pursue it.
3. Be decisive. I’ve seen too many times patients crash while “decisions were being made”. If you choose not to intervene that’s fine, but not intervening should never be the default decision, as a result of indecision. That is unacceptable. First do no harm, does not mean do nothing. Don’t fall victim to being more comfortable with the devil you know than the devil you don’t. Understand that sometimes not taking a risk can be extremely risky.
4. Learn to control your mind in stressful situations. Adrenalinization is normal. While it’s a natural reaction and will enhance your performance, too much will impair your thought process and technical skills. Learn to recognize when you’re becoming over-adrenalized, and learn whatever it is that works for you to be able to relax, stay calm, and temper your sympathetics.
5. Be cognizant of human factors. So much of what we do is psychological. Be aware of your susceptibility to cognitive bias. The key to conquering cognitive errors is to be aware of their existence.
6. Debrief after codes or tough cases and take time to reflect back after shifts. I do this routinely and I find it to be invaluable. Some of the greatest things I have picked up on have been via this process.
7. Learn Emergency Ultrasound.Believe me when I tell you that Emergency Ultrasound will transcend your practice. If you don’t learn EM ultrasound, at least learn the critical care stuff. If you don’t learn the critical care stuff, at least learn basic Echo – it has the greatest impact.
8. Follow up on your patients. I can’t express how much of my learning is through following up on my patients. If you don’t do it already – start! You will be amazed by how much you will learn.
9. Accept and embrace that some of your patients will have bad outcomes or die no matter what you do – but never, ever let this be an excuse to provide anything less than the best care you possibly can.
10. Be kind and compassionate. When it’s all said and done our patients may not remember details of their ED stay during what might very well have been the worst day of their lives – but they will remember how we made them feel.
English
@Damian_Roland @Damian_Roland I also mentioned your story on my "shop floor" last week. Must be an epidemic of lego ingestion.
English

Finally I’ve managed to legitimately say “I never found my Lego head” on the shop floor.
Leicester, England 🇬🇧 English
David Krieser retweetledi

Nice to see the 4th edition in print! Thanks to all the contributors….

English
Increase funding for General Practice so all Australians can access a GP when they need to - Sign the Petition! chng.it/HHSkm7Rx via @ChangeAUS
English
Star Trek’s William Shatner has joined the urgent call to world governments to protect half the Earth. They’re meeting right now. Up to a million species are facing extinction. Add your name now and RT. #COP15 #ForNature #biodiversity fb.avaaz.org/campaign/en/pr…
English
I'm doing the WalkWest Virtual Landmarks Challenge to support care for cancer patients in Melbourne's west! Please support my 42km, 21 day challenge. walkwest.com.au/s/1531/4359/t
English
Document a differential diagnosis.
Reduce diagnostic error.
Dr Sharon Anne McAuley #DFTB22
English
Quality Improvement: The path from "work as done" to "work as imagined"
1. Develop a Quality Mindset
2. Learn from your Team
3. Have a Data Plan
4. Use a Structured Approach
PLAN DO STUDY ACT
Thanks to @NaomiSpot #DFTB22
English
Paediatric Burns Session @DFTBubbles #DFTB22
Remember your cold water tap for Burns First Aid. 20 minutes with cold running water within the first 3 hours of the burn
English

Torn between #DFTB22 & #ASAFNA22 #Aeromed22 today - tweeting some aeromed learnings from @RFDS_CO_EGMMRS upstairs, follow all the hashtags for so much good content today!
Royal Flying Doctor Service SA/NT Aeromed Teams@rfdsSANT_EGMMRS
And we’re off! Conference opening, led by @aeromedsociety @ @FlightNurses presidents Di & Colleen. Almost 300 delegates, our first in person since 2019 - let’s do this! #ASAFNA22 #Aeromed22
English
David Krieser retweetledi

Such a privilege to listen to the inspiring Prof Franz Babl talking about network research through @PREDICT_network #DFTB22
PREDICT network@PREDICT_network
Our Grand Poobah Prof Franz Babl #DFTB22
English
David Krieser retweetledi


English
David Krieser retweetledi

After a solid week of Australian schooling for my kids, I can say that my second favourite thing about schools here is school uniforms. It's amazing to not have to worry about outfits.
Of course, that's a distant second to the fact that they won't die in a shooting.
English
@thefrancis6 talking about Rheumatic Heart Disease training in Timor Leste as an example of thinking beyond our borders. For more inspiration read or listen to this abc.net.au/radio/programs… @DFTBubbles @andrewjtagg @heartfulpaeds
English
Ulysses by Alfred, Lord Tennyson “I am a part of all that I have met”
@DFTBubbles @heartfulpaeds Transactive Memory Systems in poetry poetryfoundation.org/poems/45392/ul…
English
@BeckyPlatt3 @sintydavid @DrKanaris EZ-IO do include a triangular dressing with a mobile sleeve that will accommodate most positions. Also REALLY sticky! It allows me to place my gloved fingers adjacent to the needle to feel for extravasation.
English

@sintydavid @DrKanaris The needle should stand firm if it’s in. The syringes support it either side and the tape goes over the barrels of the syringes. I don’t tend to tape over the hub
English
Need to tape in an intraosseous needle?
No IO dressings or needle too long for the hub to sit on the skin?
Try this 👇
- Gauze with a snip in around the needle
- 2 syringes to support (size according to needle length)
- Tape firmly

English
@andrewjtagg This is a good question @andrewjtagg I was taught this by a Canberra Hosp midwife as a Junior Reg. It was a graded program: step 1: taught disposable nappy technique; step 2: cloth nappies. She had a mannequin for the initial phase before we graduated to real babies.
English
Actual question...
How many trainees (without children of their own) have ever been formally trained on how to put on a nappy/diaper?
Let's throw some sh!t around and see what sticks
Come to our neonate course on the 7th and 8th of February?
dftbdigital.com

English