Sabitlenmiş Tweet

Precision medicine can’t scale with today’s workflows.
Data is growing exponentially.
But human time isn’t.
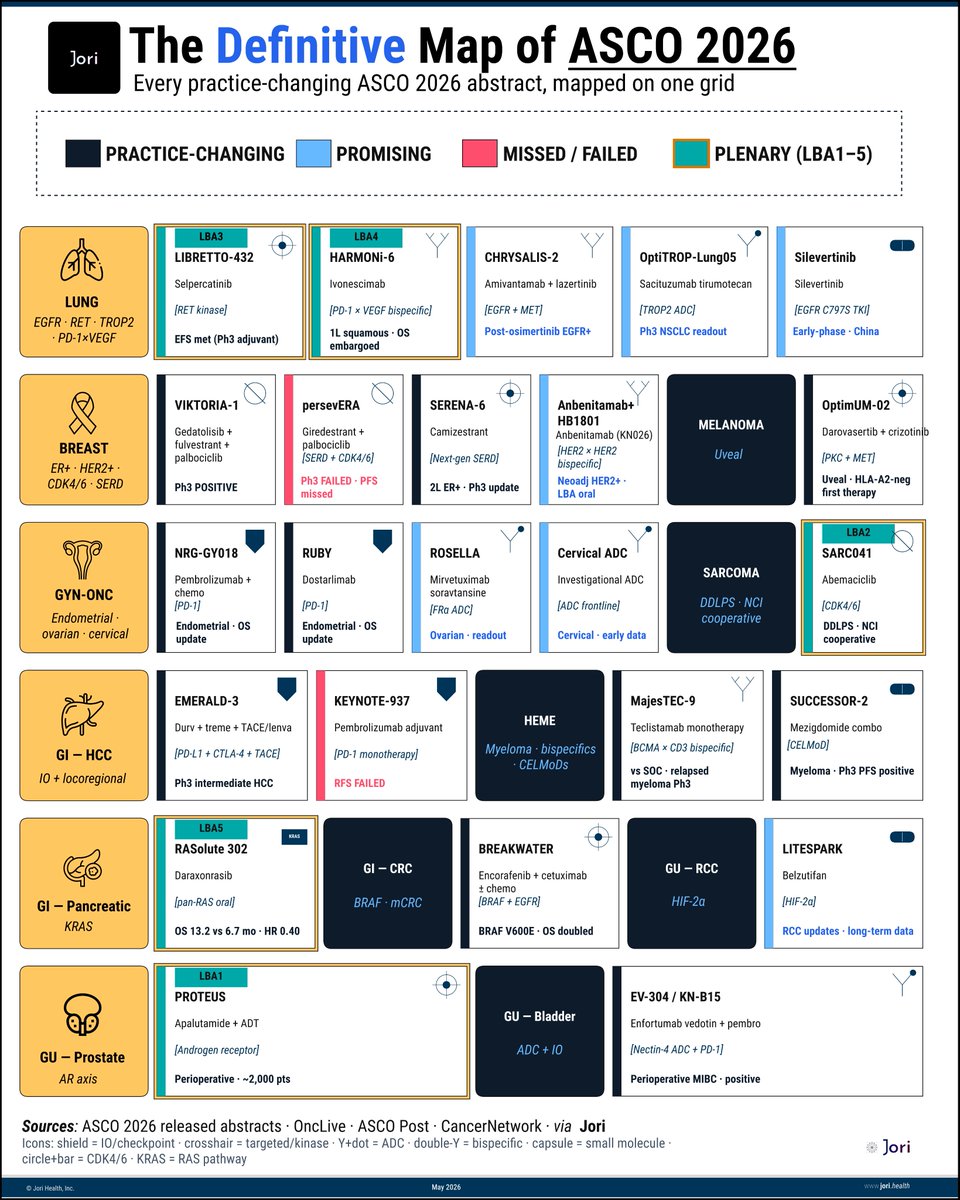
At @jori_health, we built a multi-agent system for tumor boards.
They think together. Learn together. Act fast.
40 hrs of human work → 5 mins.
Every run makes them smarter.
Every oncologist shapes the system.
Agents as infra.
This is how precision medicine scales to everyone.
English