
Luis Felipe Rivera, MD
944 posts

Luis Felipe Rivera, MD
@lfriv5
Primary Care Physician | Researcher. 🇵🇦
Panama City, Panama Katılım Nisan 2019
836 Takip Edilen204 Takipçiler

@Argenpoirot La mejor expresión de: NO tener pensamiento crítico. Vivimos millones de años en la sabana africana. El sol es, LITERALMENTE, la fuente de energía primordial del sistema planetario donde vivimos.
Sin embargo esta gente lee 3 libros manipulados y ya cree que el sol es el demonio
Español

Luis Felipe Rivera, MD retweetledi

this is actually insane
> be tech guy in australia
> adopt cancer riddled rescue dog, months to live
> not_going_to_give_you_up.mp4
> pay $3,000 to sequence her tumor DNA
> feed it to ChatGPT and AlphaFold
> zero background in biology
> identify mutated proteins, match them to drug targets
> design a custom mRNA cancer vaccine from scratch
> genomics professor is “gobsmacked” that some puppy lover did this on his own
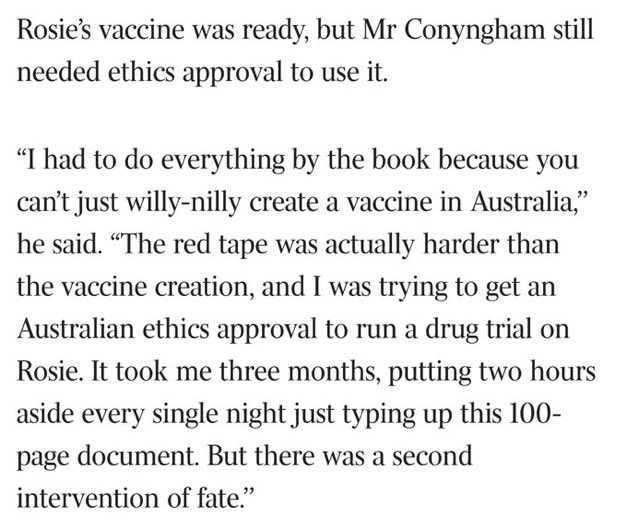
> need ethics approval to administer it
> red tape takes longer than designing the vaccine
> 3 months, finally approved
> drive 10 hours to get rosie her first injection
> tumor halves
> coat gets glossy again
> dog is alive and happy
> professor: “if we can do this for a dog, why aren’t we rolling this out to humans?”
one man with a chatbot, and $3,000 just outperformed the entire pharmaceutical discovery pipeline.
we are going to cure so many diseases.
I dont think people realize how good things are going to get



Séb Krier@sebkrier
This is wild. theaustralian.com.au/business/techn…
English
@Light_onchain @stats_feed you hace no idea what you’re talking about.
English

@stats_feed What these three have in common: all experienced either hyperinflation, extreme monetary instability, or complete loss of public trust in their own central bank.
English
Countries that use another country’s currency without formal agreement:
1.Zimbabwe 🇿🇼
2.Panama 🇵🇦
3.El Salvador 🇸🇻
English
Luis Felipe Rivera, MD retweetledi

Now that everyone is an expert on curing pancreatic cancer in mice, not rats - I want to add some context that goes beyond the headline.
You will want to read this.
Cancer is cured in mice all the time.
Thousands of times. ~90% of those “cures” fail in humans.
Why?
Because mice are:
Genetically simpler.
Treated earlier.
Short-lived.
Not humans.
Mice are a filter - not a finish line.
Yes, this study matters. It comes from the Spanish National Cancer Research Centre.
Yes, it’s pancreatic cancer - one of the deadliest there is. Yes, full tumor regression is impressive.
But here’s what it actually means:
“This approach is now good enough to risk years, trials, and millions of euros on.”
Not:
“Cancer is solved.”
What happens next?
More animal work.
Toxicology.
Phase I (safety).
Phase II (maybe works).
Phase III (beats standard care?).
Maybe 8-10 years if everything goes right.
The real damage isn’t failed drugs.
It’s failed expectations.
Every “cured cancer in mice” headline trains the public to believe:
Cures are being hidden.
Progress should be fast.
Scientists are lying when reality hits.
That’s how trust erodes.
Bottom line:
This is how real cancer progress looks.
Messy. Slow. Risky. Incremental.
Not miracles.
Not conspiracies.
Just science - doing the hard work.
✦✦✦ 𝙿𝚊𝚖𝚙𝚑𝚕𝚎𝚝𝚜 ✦✦✦@PamphletsY
🚨🇪🇸 BREAKING — Spanish Scientists Cured Pancreatic Cancer in Rats.
English



Luis Felipe Rivera, MD retweetledi

Luis Felipe Rivera, MD retweetledi


Luis Felipe Rivera, MD retweetledi

Todo mi tuiter se divide en venezolanos festejando la caída de Maduro y comunistas que viven en países democráticos llorando.
Español
Luis Felipe Rivera, MD retweetledi

The academic life sciences have normalized calling grown men and women well into their 30s and 40s “trainees.” That language infantilizes highly skilled professionals and sustains a hierarchy where those at the bottom are paid very little.
The solution isn’t simply to pay “trainees” more. The problem is that training lasts far too long.
Living on a graduate stipend in your early to mid-20s is workable. You have roommates. You carpool. You don’t eat out much. When science is your passion, you don’t need much else.
If you’re still being called a trainee in your 40s, with children, a mortgage, and the need to save for retirement, the model collapses.
The fix is earlier career paths, earlier independence, and shorter training pipelines. We shouldn’t keep people in permanent apprenticeship. We should let them become professionals while they still have a chance to build a real life.
Gokul Rajan@gokulrajan_
I have an opinion here: science is absolutely not just another job; science is passion *but* maybe pay your trainees like it is "just another job"? Because passion can't pay their bills.
English
Luis Felipe Rivera, MD retweetledi
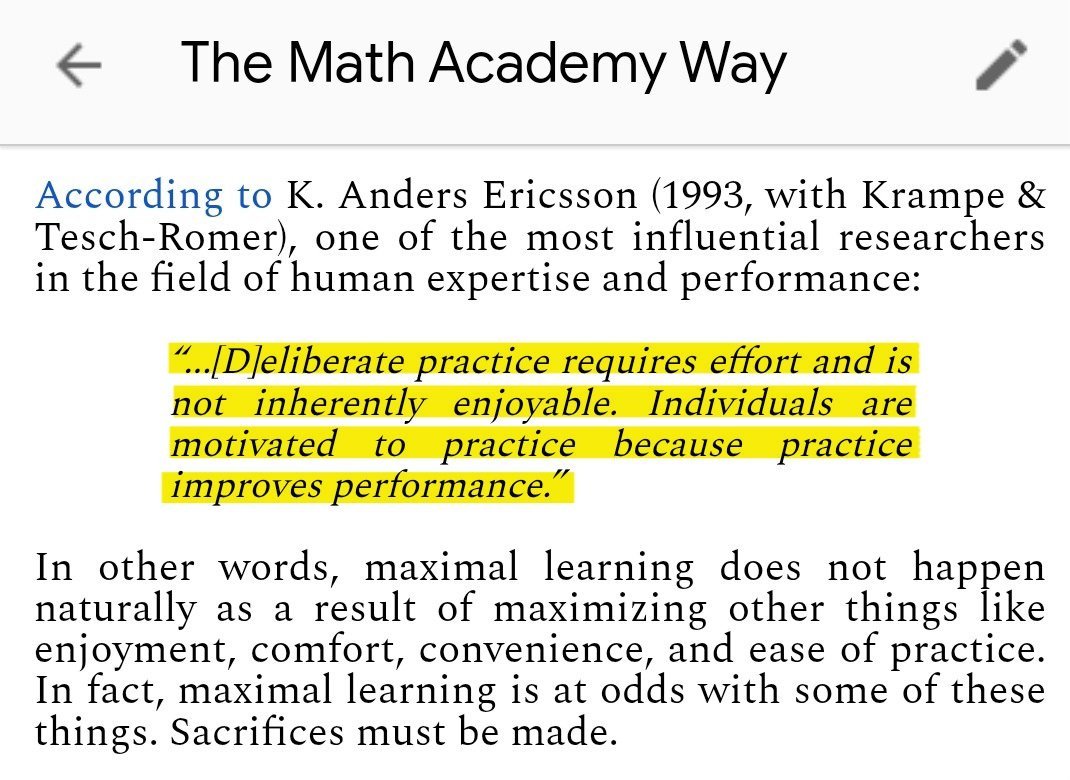
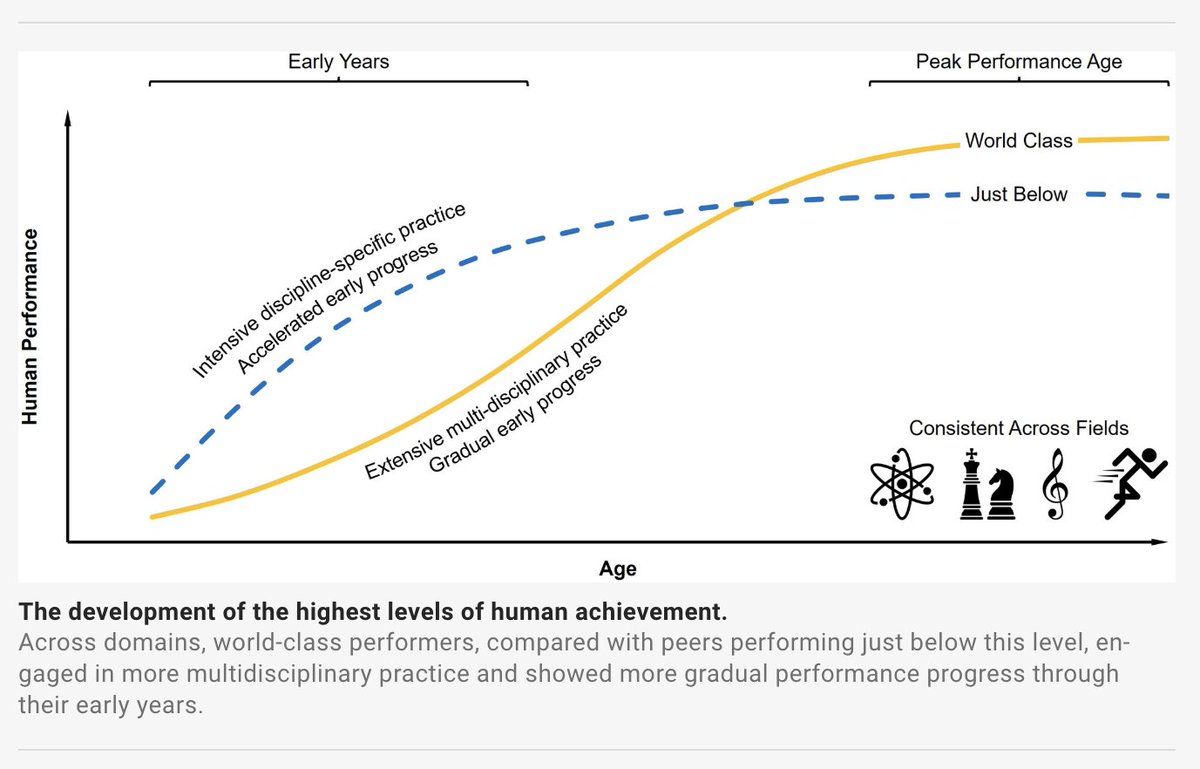
The most hard-hitting 2 sentences in all of talent development research:
Alex Hormozi@AlexHormozi
Everything is hard and no one cares.
English
Luis Felipe Rivera, MD retweetledi

Luis Felipe Rivera, MD retweetledi

I translated this into English for everyone to read. This is written by an orthopedic surgeon colleague in Spain, but I know my American colleagues will appreciate the text an similarities to challenges we face here
1/
The Asymmetry in Medicine in Spain: Responsibility Without Authority (I)
Opinion
Francisco J. Guitián Lema
The Asymmetry in Medicine in Spain: Responsibility Without Authority (I)
“There is irrefutable empirical proof of this asymmetry: the doctor can replace anyone; no one can replace the doctor,” states Francisco J. Guitián Lema, a Vigo-based traumatologist specializing in orthopedic surgery
There is a truth so elementary that it feels uncomfortable to state it: a hospital exists solely and exclusively to cure the sick. It is not there to provide jobs or to justify organizational charts. Nor to feed bureaucracies or to experiment with organizational theories. It exists so that a sick human being leaves it less sick or, at the very least, having received the best possible treatment.
From this premise follows a logical consequence that the Spanish healthcare system seems determined to ignore: in that healing process, there are only two absolutely indispensable figures. The patient, who is the reason for the entire structure’s existence, and the doctor, who possesses the knowledge to guide that process. Everything else — and this is not disdain, but taxonomy — is support structure. Necessary, valuable, often heroic, but auxiliary.
The doctor is the only professional capable of performing the core act that justifies the hospital’s existence: diagnosing the disease and establishing the treatment. Without a diagnosis, there is no possible direction. Without a therapeutic indication, there is no meaningful action. An orderly transports the patient, but it is the doctor who determines where and why. A nurse administers medication, but it is the doctor who decides which, how much, and when. A technician performs a test, but it is the doctor who orders it and interprets its result.
This functional hierarchy is not a social convention or an inherited privilege: it is a direct consequence of training. Six years of medical school plus four or five years of MIR specialization produce a professional capable of integrating knowledge of anatomy, physiology, pathology, pharmacology, and a thousand other disciplines into a diagnostic synthesis that no other healthcare professional is trained to perform.
There is irrefutable empirical proof of this asymmetry: interchangeability. A doctor can, in case of need, perform the functions of any other hospital professional. They can push a stretcher, insert an IV line, draw blood, take vital signs — in Germany, doctors routinely perform these functions. The reverse is not true. An orderly cannot diagnose pneumonia. A nurse cannot order a surgical intervention. The doctor can replace anyone; no one can replace the doctor.
Recognizing this reality does not imply disdain toward anyone. Nursing care is essential. The orderly’s work ensures that hospital flow does not stop. Everyone deserves respect and fair compensation.
But respect for personal dignity cannot be confused with functional equivalence. In an operating room, the surgeon is not worth more as a human being than the assistant; but their function is irreplaceable in a way that the assistant’s is not.
This distinction, obvious in any other field, has become taboo in Spanish healthcare. The prevailing egalitarianism has managed to make an evident functional truth be perceived as a moral offense.
Angel L. Rodríguez@angelluisamyts
"un hospital existe única y exclusivamente para curar enfermos. No sirve para dar empleo ni para justificar organigramas. Tampoco para alimentar burocracias ni para experimentar teorías organizativa" Gran artículo, merece la pena leerlo. farodevigo.es/opinion/2025/1…
English
Luis Felipe Rivera, MD retweetledi

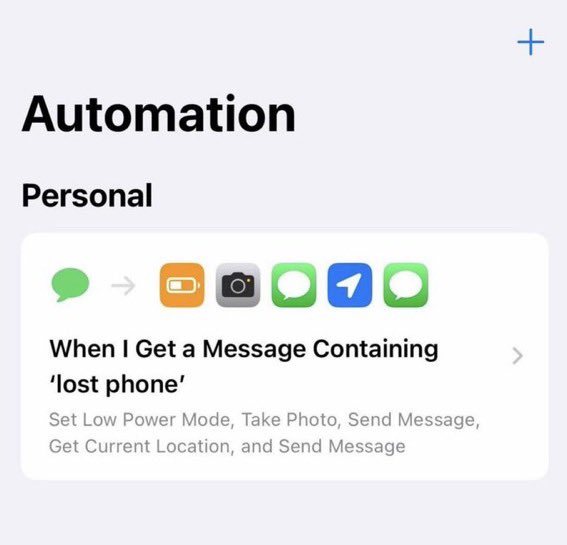
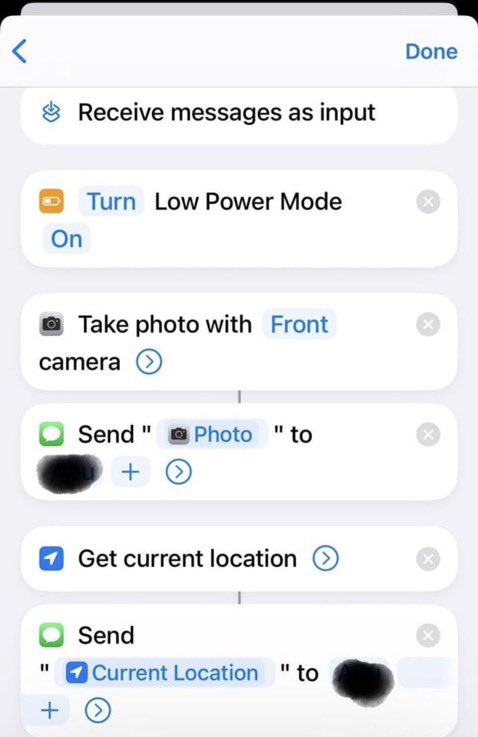
If your phone goes missing, you can easily see who stole it and exactly where it is
- Open Shortcuts and select Automation.
- Then tap Create Personal Automation.
- Choose Message and set a trigger word (example: LOST)
Actions (in this order):
• Set Low Power Mode → ON
• Take Photo → Front camera (preview OFF)
• Get Current Location
• Send Message → your number (photo + location)
Turn Ask Before Running → OFF
Turn Notify When Run → OFF
Anytime that keyword is sent from any phone, it runs automatically.
Isabella@BchNinja4
Just found my phone after losing it 24 hours ago 😭
English
Luis Felipe Rivera, MD retweetledi


@nayibbukele domestic abuser nonsense logic right here, pretending like the only two options are run an inhumane prison that violates human rights or no prison at all
English

Madam Secretary Hillary Clinton,
If you are convinced that torture is taking place at CECOT, El Salvador is ready to cooperate fully.
We are willing to release our entire prison population (including all gang leaders and all those described as “political prisoners”) to any country willing to receive them.
The only condition is straightforward: it must be everyone.
This would also greatly assist journalists and your favorite NGOs, who would then have thousands of former inmates available for interviews, making it far easier to find additional voices critical of the Salvadoran government (or willing to confirm whatever conclusions are already expected).
Surely, if these testimonies reflect a systemic reality, a much larger pool of sources should only reinforce the claim, and many governments should be eager to offer protection.
Until then, we will continue prioritizing the human rights of the millions of Salvadorans who today live free from gang rule.
Respectfully,
Nayib Bukele
Hillary Clinton@HillaryClinton
Curious to learn more about CECOT? Hear Juan, Andry, and Wilmer share firsthand how the Trump administration branded them as gang members without evidence and deported them to the brutal El Salvadoran prison. youtube.com/watch?v=Lku5h9…
English
Luis Felipe Rivera, MD retweetledi

A massive new study on peak performance included 34,000 international top performers: Nobel laureates, renowned classical music composers, Olympic champs, and the world’s best chess players. It shows early specialization is a trap, and the road to greatness is long and varied.
English
Luis Felipe Rivera, MD retweetledi

Luis Felipe Rivera, MD retweetledi


Luis Felipe Rivera, MD retweetledi
