Seja aprovado na base do time do seu coração.
Mas, ainda moleque, seja dispensado por “baixa estatura”.
Se frustre. Se medique. Vá para o rival.
Se destaque na base, vire referência na Seleção.
Se profissionalize, brilhe em um ano como titular e acerte com o Real Madrid.
Rompa o ligamento cruzado e veja o sonho europeu desabar.
Depois de 7 meses fora, dê a volta por cima.
Veja o clube do seu coração te desejar novamente.
Se reúna com o presidente, chore, mostre paixão, implore pra ser negociado…
e ainda assim se sinta contrariado. Vá para a Itália.
Não se adapte à Europa.
E, quando ninguém mais espera, realize o sonho: vista a camisa do Flamengo como profissional.
Ganhe títulos. Faça história. Vire titular absoluto.
Seja o Camisa 9. Seja o P9.
E, contra o ex-clube que um dia te contrariou…
Marque dois golaços, exploda a torcida e se consagre, disparadamente, como o maior artilheiro do Flamengo no século XXI.
Pedro Guilherme. O P9.
Lembro exatamente desse lance, pau quebrando no meio da bateria da torcida.
Pablo e Benfica discutindo pra crl kkkkk do nada gol e os cara se abraça kkkkkkkkkkkkkkkkkkkkkkkkkkkkk
Em terra de Messi, quem é Galinho é REI👑
Essa semana, muitos enzos, oportunistas ou até mesmo ignorantes quando o assunto é futebol, surfaram na onda para criticar o Zico porque ele “ousou” dizer que fazia as coisas que o Messi faz (ou fazia também).
Deu trabalho, mas reunimos depoimentos de grandes figuras do futebol e do jornalismo esportivo - incluindo Pelé, Tite, Galvão Bueno, Vampeta, Mauro Cezar, Djalminha e muitos outros - reverenciando o maior ídolo da história do Flamengo e um dos maiores jogadores de futebol que esse mundo já viu.
Concorde ou não, mas a verdade foi dita: o Zico está na prateleira dos maiores de todos os tempos do futebol... para despeito dos antis.
Criticar o Zico por não ter ganhado um título que é disputado apenas de 4 em 4 anos, sendo que foi garfado em 78, merecia demais ganhar em 82 e foi machucado em 86*, ou por não ter jogado muito tempo na europa**, sendo que aqui se praticava o melhor e mais competitivo futebol do mundo à época, é puro recalque ou vira-latismo.
Enfim, o que deve doer para eles é não ter um ídolo da envergadura do Zico. Seja do ponto de vista do futebol. Seja do ponto de vista moral.
Esse Adm tem muito orgulho de ter o Zico como maior ídolo! E tenho certeza que 99% da Nação também! Se é o seu caso, diga de onde é e deixe seu MUITO OBRIGADO ao @zico
Vídeo em 4K no YT. Link nos stories e canal de transmissão aqui do Insta. É muito importante que curtam e comentem no vídeo lá para chegar a mais pessoas. Zico merece! @Galinho1953#Zico#GalinhodeQuintino#ReiZico#NataldoFlamenguista#galinho#camisa10dagávea
*(e ainda assim entrou e gerou a jogada do pênalti que ele perdeu... Se não tivesse entrado teria ido para os pênaltis igualmente. E nas cobranças ele fez o dele. Sócrates perdeu. Mas aí ninguém lembra.)
**(mesmo assim no ano que jogou na fraca Udinese não foi artilheiro por um gol no italiano, perdendo para o Platini que tinha muito mais jogos).
❤️🖤@mundobolaFlamengo@zinho@vampetaoficial@Andrerizek@benjaminback@galvaobueno@edsonmauro1@muller7oficial@Ronaldo@MuricyRamalhoRe@Petkovic10@edmundosouza7@SilasCoach@maurocezar
Summary of all Late-Breaking Trials at #ACC2026 – take home points
@ACCinTouch@ACCmediacenter@JACCJournals
1. HI-PEITHO: Ultrasound-facilitated catheter-directed thrombolysis led to a lower risk of PE-related death, cardiopulmonary decompensation or collapse, or recurrence of PE. vs anticoagulation alone in intermediate-high risk PE.
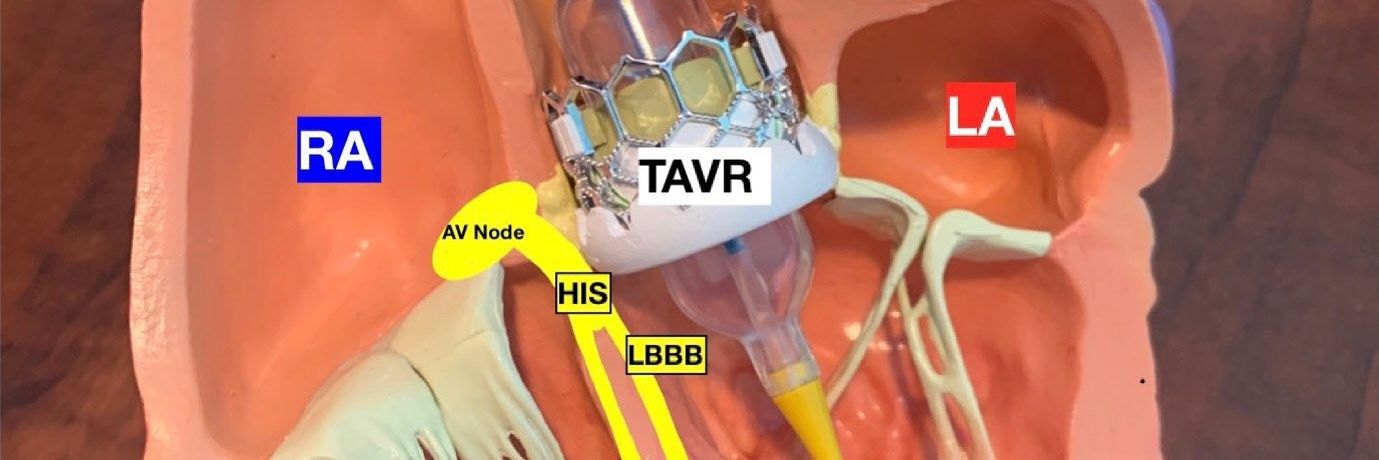
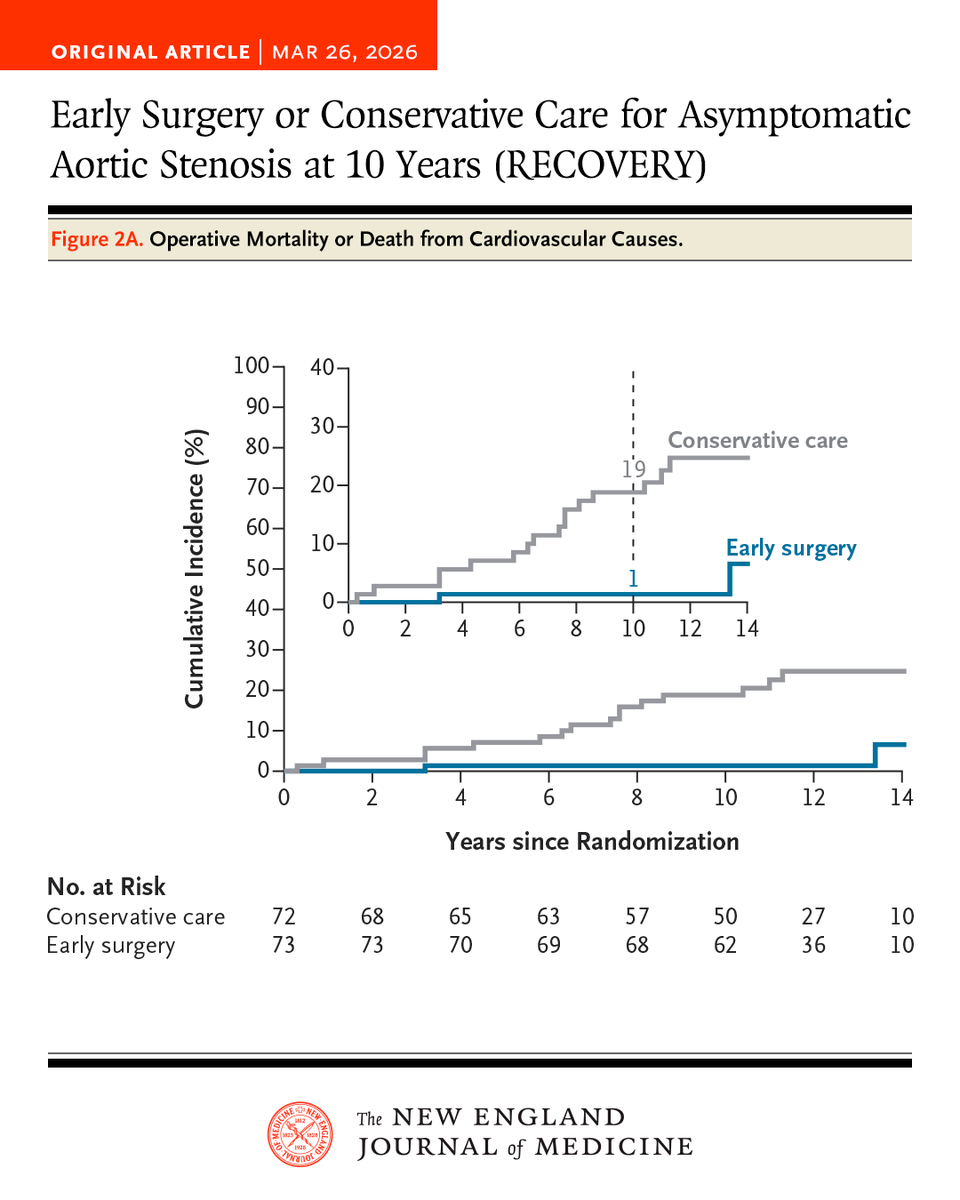
Early surgery in asymptomatic patients with very severe aortic stenosis led to a lower risk of a composite of operative mortality or death from cardiovascular causes at 10 years than conservative care. Full RECOVERY trial results: nejm.org/doi/full/10.10…
A one-time midlife assessment of four blood-based biomarkers—CAD polygenic risk score (PRS), hsCRP, LDL-C, and lipoprotein(a)—robustly predicts future coronary artery disease risk in both men and women aged 40 to 69 years.
A one-time midlife biomarker panel may unmask hidden future CAD risk long before conventional calculators do.
🔹 Pearl 1 — Four pathways, one practical panel
A single midlife assessment of CAD polygenic risk score (PRS), LDL-C, lipoprotein(a), and hsCRP captures genetic, lipid, and inflammatory risk, offering a more integrated view of future coronary artery disease risk.
🔹 Pearl 2 — Each biomarker independently predicts incident CAD
Over 12 years of follow-up, elevation of each biomarker was independently associated with higher CAD risk. The hazard ratios were 1.79 for CAD PRS, 1.60 for LDL-C, 1.20 for Lp(a), and 1.64 for hsCRP, confirming that all four add meaningful prognostic information.
🔹 Pearl 3 — Risk is multiplicative, not merely additive
Individuals with all four biomarkers elevated had a 4.65-fold higher risk of future CAD compared with those with no elevated biomarkers, highlighting the importance of cumulative burden across pathways.
🔹 Pearl 4 — Younger adults may benefit the most
All four biomarkers showed stronger associations at younger ages, suggesting that biomarker-based screening may be especially valuable in early midlife, when traditional clinical calculators often underestimate lifetime vascular risk.
🔹 Pearl 5 — Biomarkers can rival traditional risk calculators
The combined 4-biomarker model achieved a C-statistic of 0.753, which was slightly better than the pooled cohort equations at 0.740, indicating comparable or better discriminatory performance.
🔹 Pearl 6 — Better reclassification means fewer missed patients
Compared with pooled cohort equations, the 4-biomarker strategy produced a 32% continuous net reclassification improvement, suggesting it may identify at-risk individuals who would otherwise be missed by conventional clinical scoring.
🔹 Pearl 7 — CAD PRS appears particularly informative in men
The association of CAD PRS with incident CAD was stronger in men than in women, although the 4-biomarker model was predictive in both sexes.
🔹 Pearl 8 — Lp(a) still matters even when effect size is modest
Although the hazard ratio for Lp(a) was lower than for the other markers, it remained an independent predictor of CAD, reinforcing the value of at least once-in-a-lifetime Lp(a) testing in risk stratification.
🔹 Pearl 9 — hsCRP keeps inflammation in the CAD conversation
The strong association of hsCRP with future CAD supports the concept that residual inflammatory risk deserves attention alongside cholesterol and inherited risk.
🔹 Pearl 10 — Think beyond 10-year risk; think lifetime vascular exposure
This study supports interpreting CAD risk as a cumulative lifetime burden of inherited susceptibility, atherogenic lipids, and inflammation, which may help clinicians prioritize earlier and more targeted primary prevention.
Practical CME INDIA Take-Home Message
In adults aged 40–69 years, a one-time 4-marker panel of CAD PRS, LDL-C, Lp(a), and hsCRP may refine CAD risk assessment beyond traditional calculators, especially in younger individuals and those who appear low-risk by routine clinical scoring. This approach may help clinicians identify candidates for earlier lifestyle intensification, lipid lowering, closer follow-up, and personalized prevention strategies.
One-Line Conclusion
Midlife CAD prevention may become smarter when we measure inherited risk, cholesterol burden, lipoprotein(a), and inflammation together—not separately.
sciencedirect.com/science/articl…
Uma boa análise de um tema polêmico na Cardiologia: A resposta da pressão arterial ao exercício varia de acordo com a capacidade física do indivíduo e isso precisa ser considerado!
cardioteca.com/hipertension-a…
🧬🫀 Lipoprotein(a) meets Calcium Score: are we finally refining risk?
This large multicohort study tackles a clinically frustrating question:
👉 What do we do with elevated Lp(a) when risk is still uncertain?
🔍 Core idea
Lp(a) is a genetically driven, causal risk factor for ASCVD.
But in practice:
⚠️ Risk remains heterogeneous
⚠️ Treatment pathways are still evolving
⚠️ Not all patients with high Lp(a) behave the same
📊 What this study shows
Adding Coronary Artery Calcium (CAC) dramatically improves risk stratification:
✅ High Lp(a) + high CAC → clearly elevated risk
✅ High Lp(a) + CAC = 0 → surprisingly lower short-term risk
👉 In other words:
Lp(a) = potential risk
CAC = realized disease
🧠 Why this matters
We often treat Lp(a) as a binary “on/off” risk signal.
This paper reinforces a more nuanced model:
💡 Risk is not just biology (Lp(a))
💡 It’s the interaction between biology + plaque burden
⚖️ But here’s the catch
Population-level conclusions can mislead:
CAC = 0 does NOT mean “no risk”
It may simply reflect earlier disease stage
Especially relevant in younger patients with high Lp(a)
👉 Time horizon matters.
🔮 Clinical takeaway
This is where imaging becomes decisive:
✔️ Use CAC to contextualize Lp(a)
✔️ Avoid over- or under-treatment
✔️ Move toward precision prevention
🚨 Bottom line
Lp(a) tells you who might be at risk
CAC tells you who already is
The future is not choosing between them—
👉 it’s integrating both intelligently
@Albumism Well, I believe Accelerate is a very good album, most underrated from their discography. Until the day is done, one of the most valuable songs ever done by the guys, came from this album...