
I am biased because I see these patients in a neuroimmunology clinic, where many progressive myelopathies are labeled as “transverse myelitis,” and delayed diagnosis is unfortunately common among them.
Typically a man >50 with slowly progressive myelopathy over months. Radicular pain is a frequent initial symptom, often presenting as chronic, insidious low back pain. Prior spine surgery is not uncommon. Symptoms may worsen with steroids or show only transient improvement. Stepwise decline with exertion/Valsalva,early gait impairment and neurogenic bladder/bowel dysfunction.
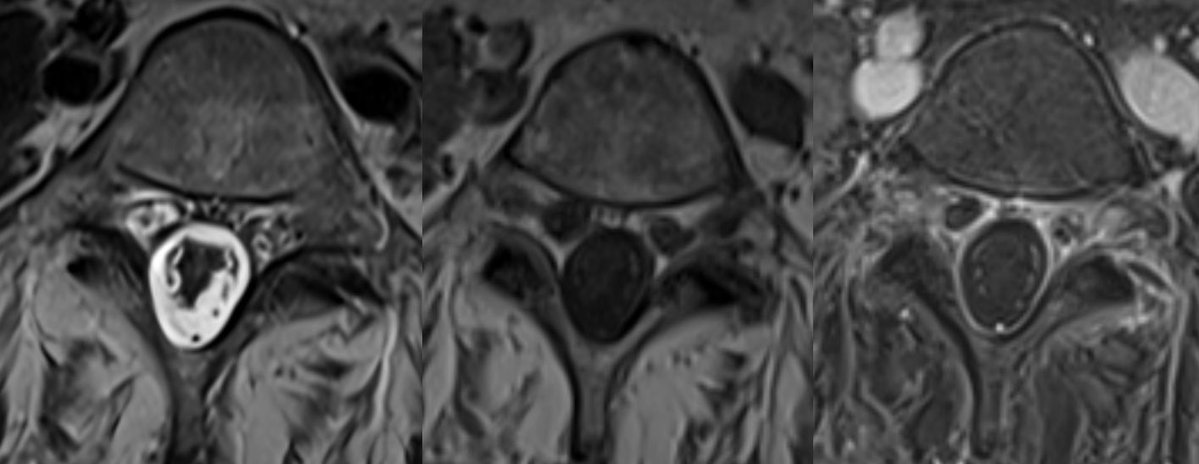
Important pitfalls: absence of obvious flow voids on MRI does not exclude the diagnosis. CSF is often abnormal (elevated RBCs protein common), but pleocytosis is uncommon.
A single spinal angiogram may be negative, some patients require repeat, highly selective angiography, and occasionally surgical exploration to localize and treat the fistula.
Any unexplained thoracic myelopathy extending to the conus should prompt a thorough evaluation for a spinal dural AV fistula.
English