
Thomas Jacques
36 posts

@drruthannharpur What about Chinese women who want to use Traditional Chinese Medicine?
English

Absolute nonsense passing as professional education and development in midwifery
James Titcombe@JamesTitcombe
“Acupressure points to support cervical ripening and labour onset…” The state of midwifery education in the NHS is dire….
English
@ClearThinker66 @kcisc @Microbedoc2 @Molly2323232323 @AlisonGeorge10 @PrimaryCareNHS @DHSCgovuk @karinsmyth @LaylaMoran @Jeremy_Hunt @DAUK_GP @BMA_GP @VictoriaTzB Doesn’t change management, we virtually never do it
English

@Microbedoc2 @Molly2323232323 @AlisonGeorge10 @PrimaryCareNHS @DHSCgovuk @karinsmyth @LaylaMoran @Jeremy_Hunt @DAUK_GP @BMA_GP @VictoriaTzB Blimey. I had a good grasp of all of that as a beginner SHO paed. My issue is people not bothering to do micro at all. I had a kid referred to ENT by their GP for recurrent tonsillitis who had only ever had one throat swab done. Don’t people want to know what bugs grow anymore?
English

@SebPillon makes a very important point!
Since the expansion of ARRS roles & therefore increasing referrals being made by non-GPs, I’ve heard that the QUALITY of REFERRALS has fallen SIGNIFICANTLY!
A consultant friend says they are being swamped by poor referrals.
@SKinnock
1/
Seb@SebPillon
My cynical side wonders that A&G is actually part of the "replace GPs" agenda. Have non doctors running primary care being remotely supervised by A&G. Specialists are great at being specialist. Primary care is largely about a holistic & generalist approach and we can't lose that
English
@cannula_service Robots are multipurpose which greatly mitigates the cost. An operating microscope can be as much as £400k remember, and robots are getting cheaper. Ask a general surgeon about the evidence base in their specialty, just as I’d ask you the evidence base for VL or TIVA!
English

@mrthomasjacques I don't know enough about ENT & robotics to comment on that. And ofc I get cost analysis is complicated.
But for routine surgeries done w/o robot like gallbladder, hemicolectomies, etc, I find evidence base lacking to justify exorbitant cost of robot.
As the NHS currently is.
English
Hahahaha, robotics reducing the wait list? Tell me you've never sat through a robotic surgery list without telling me.
A waste of money is what it is.
English
@cannula_service I, and my surgical colleagues, are smart enough to know that long anaesthetic time has associated risk. We have weighed that up and these operations are still taking place. If they are longer operations, that may well be justifiable (but we should be asked to justify it).
English
@cannula_service What I mean is: if the surgery takes longer but allows for better swallowing function, better recovery and/or complete avoidance of radiotherapy, length of anaesthesia is irrelevant to decision making. The same goes for the cost/benefit analysis - you’re oversimplifying.
English
@cannula_service Problem is you don’t establish an evidence base without doing the work. In head and neck surgery (oropharyngeal ca) there is robust evidence that we didn’t have 10 y ago. Length of anaesthesia is not an important metric.
English
@mrthomasjacques I would also say that besides a few evidence based surgeries (chiefly urology if I remember), for the many other types I see (robotic gen surg & gynae, nephrectomy) there isn't good evidence that it improves patient outcomes at all + prolonged length of anaesthesia assoc w/ risk.
English
@cannula_service In head and neck surgery, it is definitely the latter. It is absolutely not a waste of time and the same goes for Urology. But it definitely has nothing to do with waiting lists.
English
@cannula_service A clear distinction needs to be made between “converting“ existing operations to robotic ones as proof of concept, versus robotic surgery enabling approaches that previously were not possible.
English
@DrMohitBhagia ocacademy.in/blogs/foreign-…
Interesting how Indian colleges have quotas that mean foreign medical graduates are restricted from training posts back home. Almost as if this is a normal thing.
English

In other words, the doctor responsible for your NHS care may no longer be the best candidate for the job.
They may simply be the one who graduated in the UK.
I would have thought the Health Secretary would want patients treated by the best. Apparently not.
Wes Streeting@wesstreeting
I’m keeping my promise to resident doctors. We’re looking after our homegrown talent. Thanks to @fletchjack and @BMAResidents for working together with us on this.
English
@EwenPearson2 @Tom_SkinnerBC Anyone earning that much privately is LTFT on NHS. But that doesn’t diminish the point of the post I don’t think.
English

@Tom_SkinnerBC How many UK Drs is that? A tiny amount & probably zero work/life balance
English

If you’re earning £200k+ in the NHS and £500k+ in private practice,
you shouldn’t be spending your evenings at pension webinars.
Your adviser should.
If you’re juggling theatre lists, family life and a triathlon block,
you don’t need another course.
You need an adviser who already understands:
• Annual Allowance taper
• Scheme Pays strategy
• McCloud remedy
• Private/NHS interaction
• Sequencing risk in a DB world
But that's not the biggest issue. An online course can't answer:
- Do I retire at 55, 58, or 60?
- Do I take actuarial reduction or bridge?
- Do I use ISA, GIA, DC, or retained earnings?
- How do I smooth tax bands between stepping down and DB commencement?
- Should private practice earnings taper alongside NHS pension income?
Your time is better spent where you’re irreplaceable.
The rest should be delegated.
English
@ChefReactions Pied a Terre or Chez Bruce for fancy French. Savoy Grill or Beast for steak. Hakkasan or A Wong for Chinese. Cinnamon Club or Gymkhana for Indian. 😃
English


@BMA_James_Steen @BMALondon The govt won’t listen to this line of argument because LW isn’t there for the sake of *fairness*. COL varies elsewhere in the UK. You need to demonstrate London lacks applicants for jobs or they’ll ignore you. Focus on uniform salary increases instead.
English

@mrthomasjacques @BMALondon Doctors will go where the training opportunities are, yes, and London has a disproportionate number of training posts due to the number and size of the teaching hospitals.
That doesn’t mean those doctors necessarily want to live in London / wouldn’t choose to live elsewhere.
English
London Weighting for doctors is insult.
London is no cheaper for doctors, and London needs doctors just as much as it needs all these other key workers.
Now the new regional council is in place, @BMALondon will be launching a campaign to tackle this insult head on very soon.
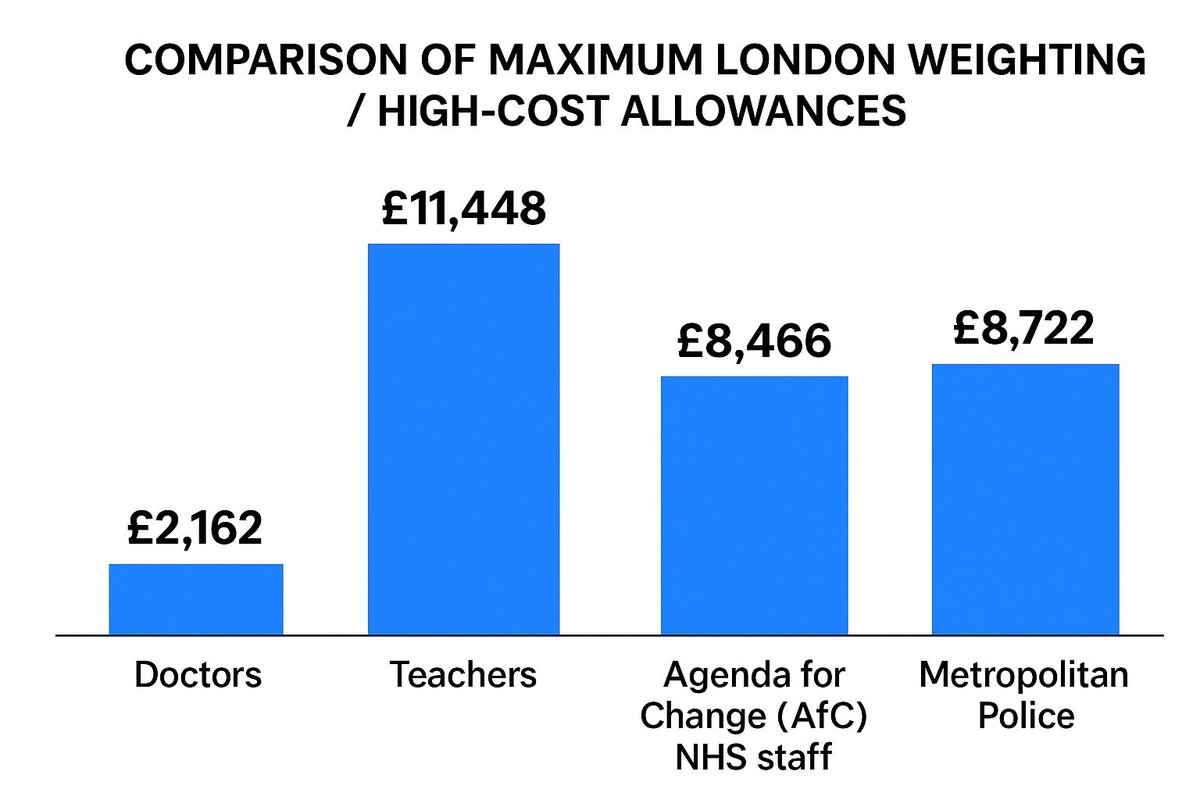
AngryDoc 🦀@angrydoc18
Disgraceful that London Weighting for doctors is less than 3 times other NHS staff Our london weighting has not increased since 2005 London doctors are being left behind @BMAResidents please can this be addressed urgently this ultimately comes down to our union
English
@BMA_James_Steen @BMALondon Furthermore the issue you’re highlighting affects the whole UK, not just London, and thus isn’t related to London weighting.
English
@BMA_James_Steen @BMALondon That’s not due to a lack of applicants though, is it? It’s a lack of positions and investment in medical staffing. You can’t complain about competition ratios as well as making this point, unless there’s a detail I’m missing.
English
@AliJaneMoore It comes down to job planning, and skewed departmental priorities that favour the 52 week elective pathway above everything else.
English

Sometimes I really, really wonder about how the NHS is run.

English