Nurten Sayar, MD retweetledi

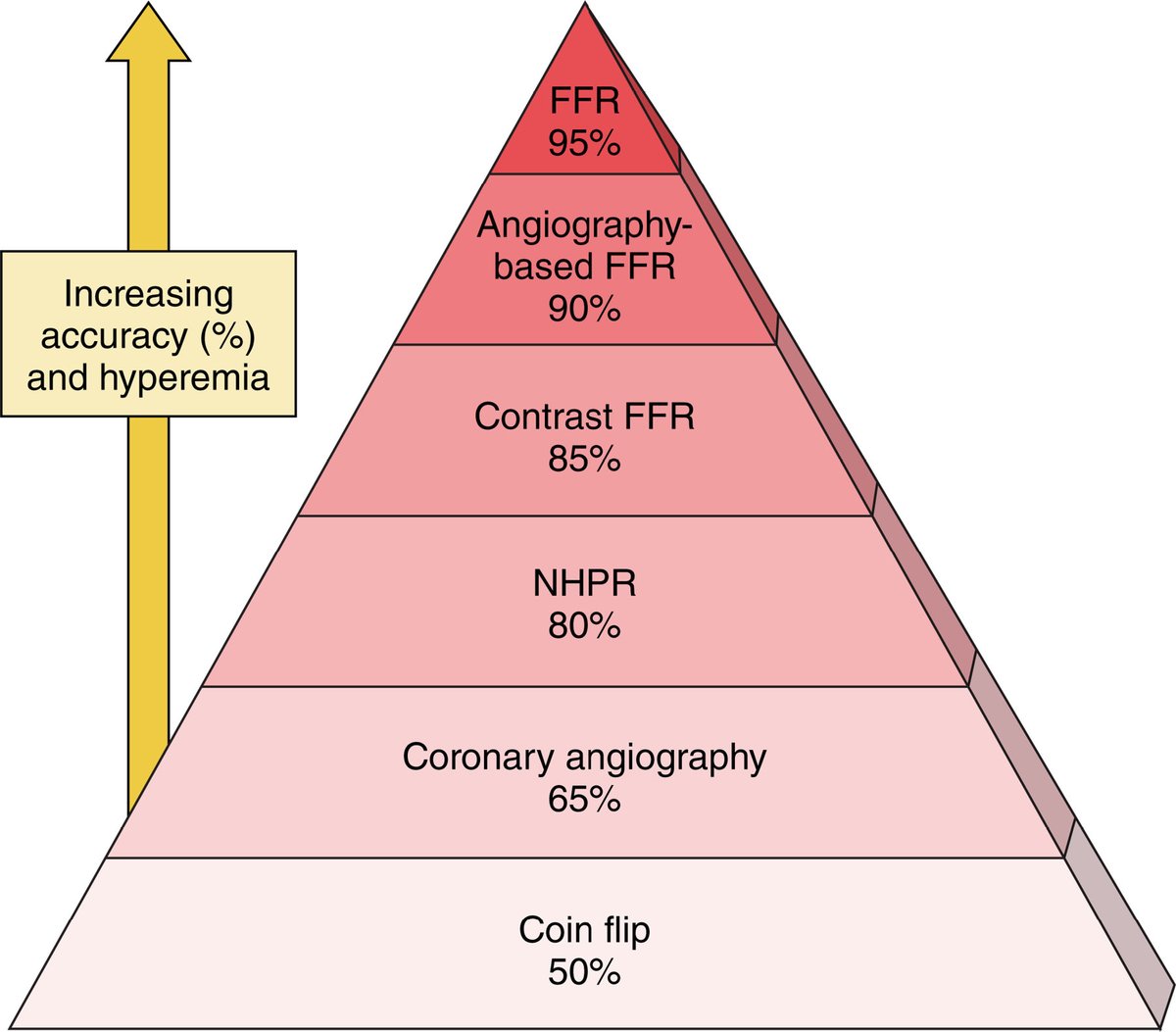
@JayMathewsMD @ShariqShamimMD @realarainmd @Hragy @jedicath @drandrewsharp @evandrofilhobr @serioustaurean @DrMarthaGulati @iamritu @IntervnCardio The concordance of FFR vs NHPR is only 80%. Agree that the better comparator is invasive FFR. Here is the pyramid of diagnostic accuracy.
English