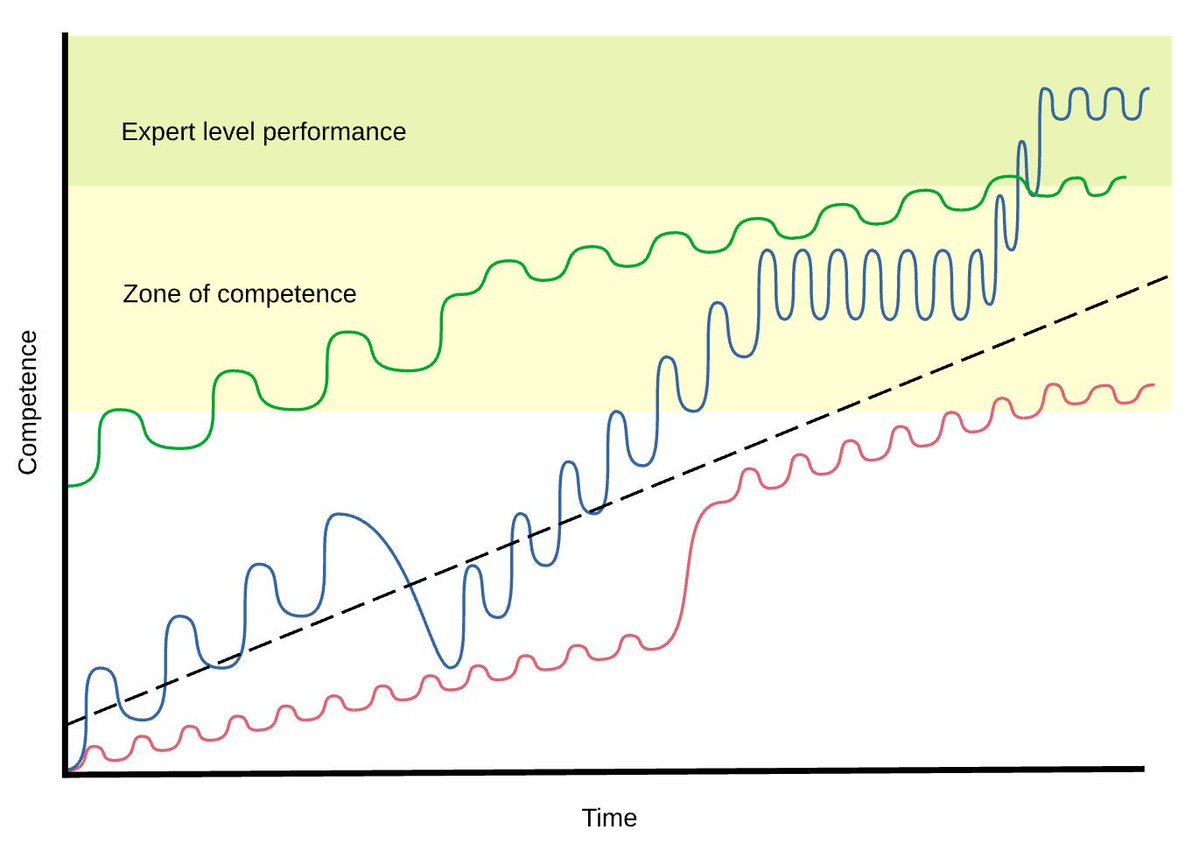
@Anaes_Journal Interesting ideal line - would have thought it would be shallow-steep-shallow sigmoid.
English
Marc Chikhani
4.7K posts

@quartered_onion
Magnesiumologist; mea sententia


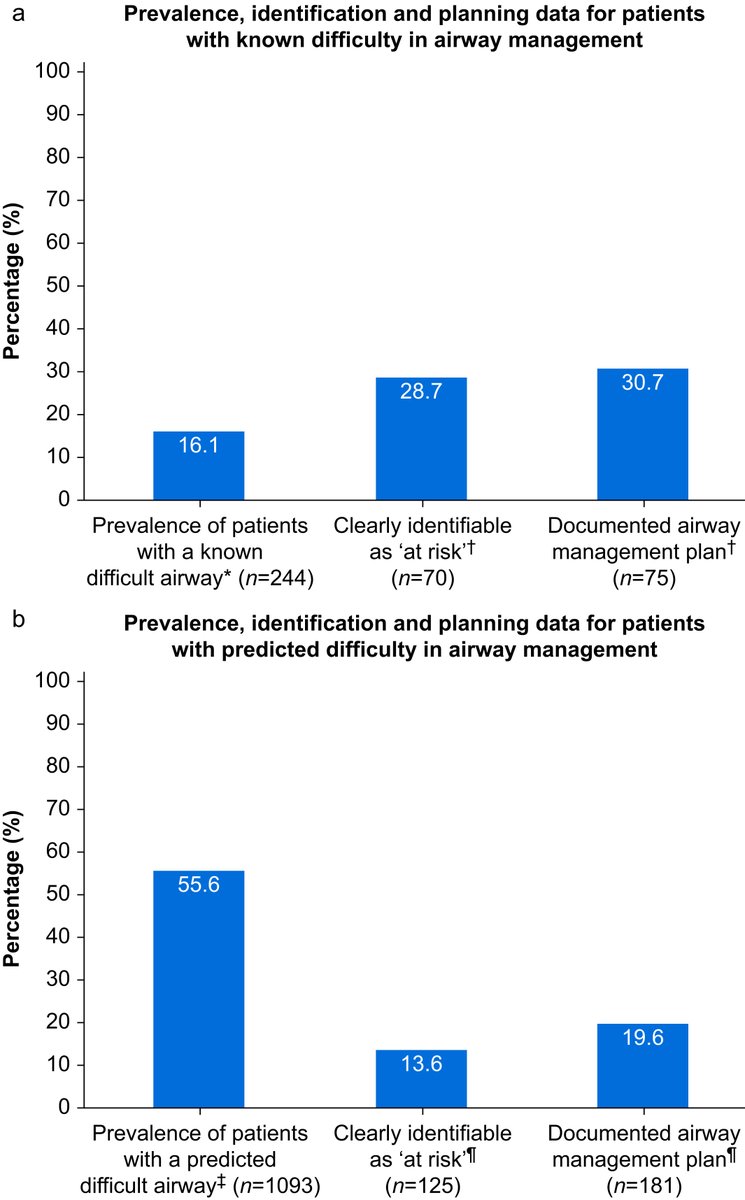
Are we missing signs of #airwaydifficulty in #criticalcare? This new study reveals gaps in recognition and planning—see the data and learn how we can improve patient safety. Read more: bjanaesthesia.org/article/S0007-…



Introducing the #VCIscore: a reliable, standardised tool for reporting #videolaryngoscopy-assisted #trachealintubation. High inter-rater agreement means better data and safer care. Read more: bjanaesthesia.org/article/S0007-…









My understanding was that the main problem with reusing propofol syringes is not contamination but that the propofol coats the inside of the syringe leading to the the pump sticking with the risk of awareness during TIVA. I never refill propofol syringes for this reason.