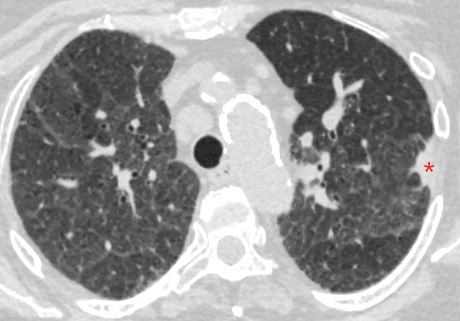
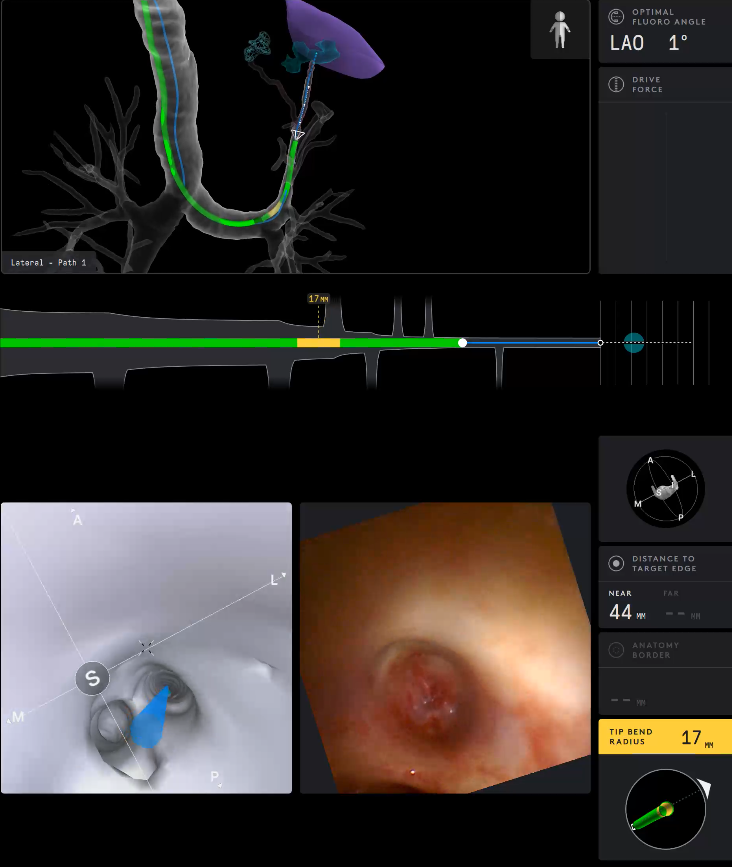
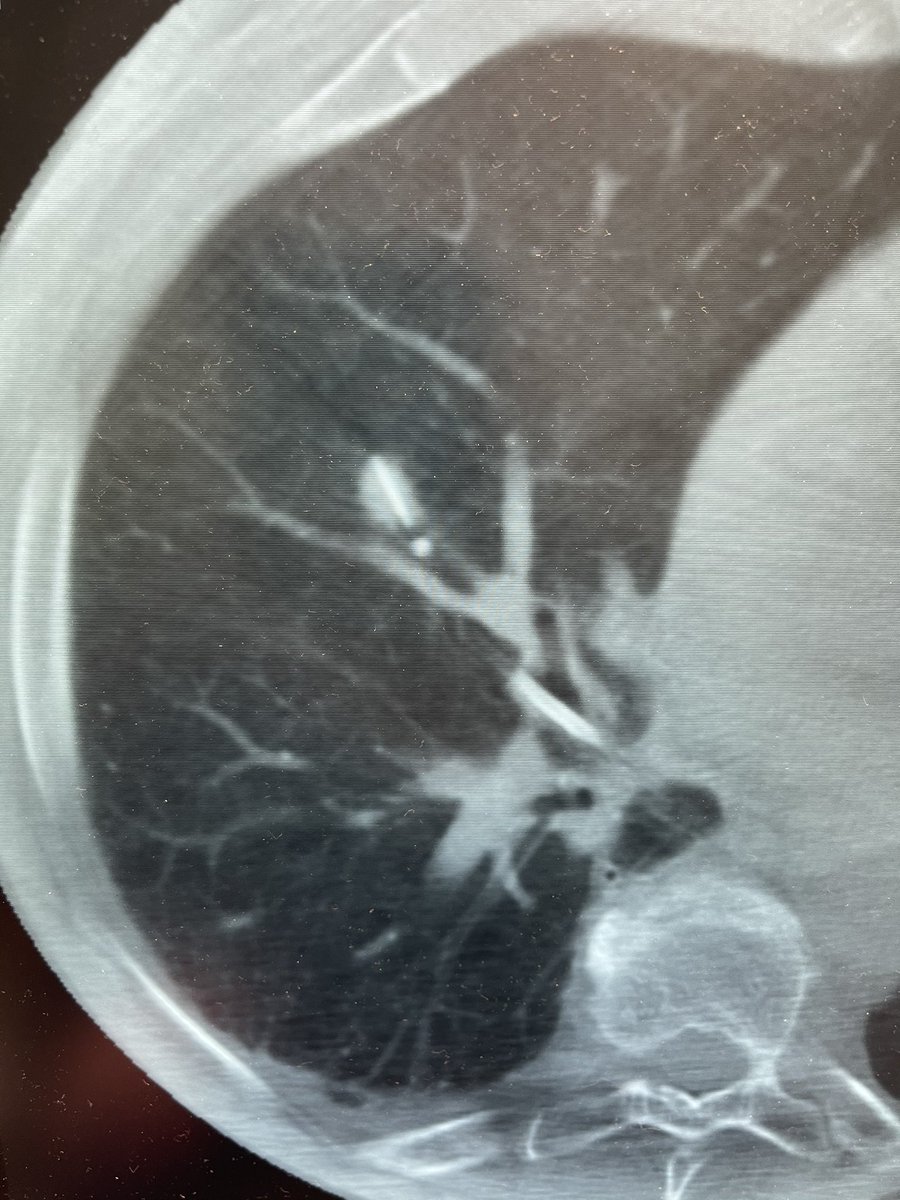
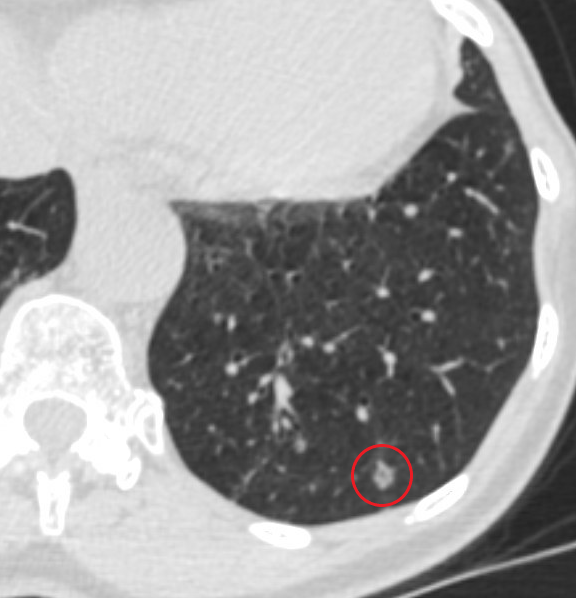
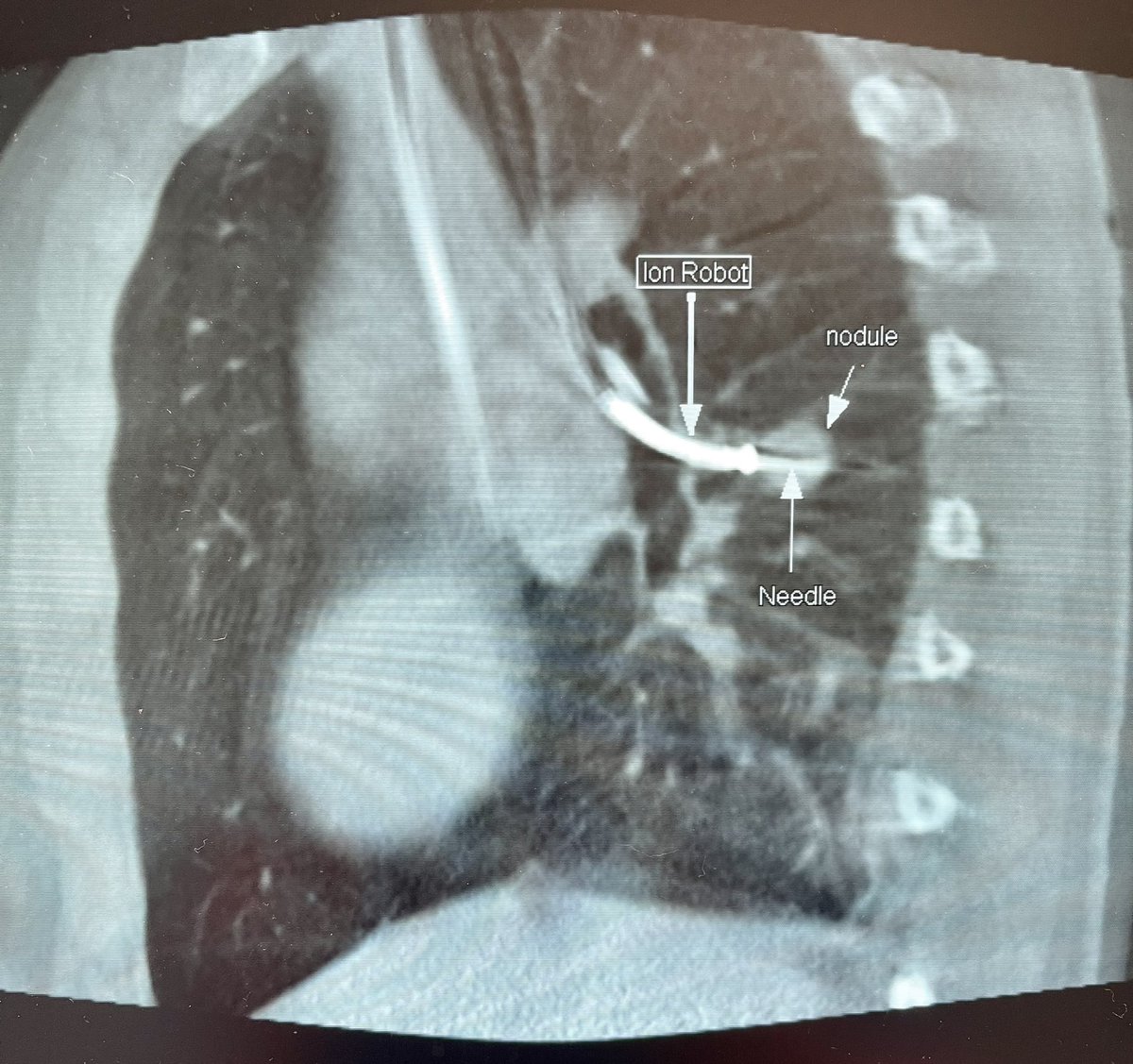
Cool case: 4.5mm partially solid PET-Avid LLL nodule. Used High PEEP/Tidal volume and wedged left side up to decrease dependent atelectasis. Navigated with Ion and adjusted with Philips CBCT. ROSE positive for Adenocarcinoma. Exciting times in lung cancer care! #ION#cbct
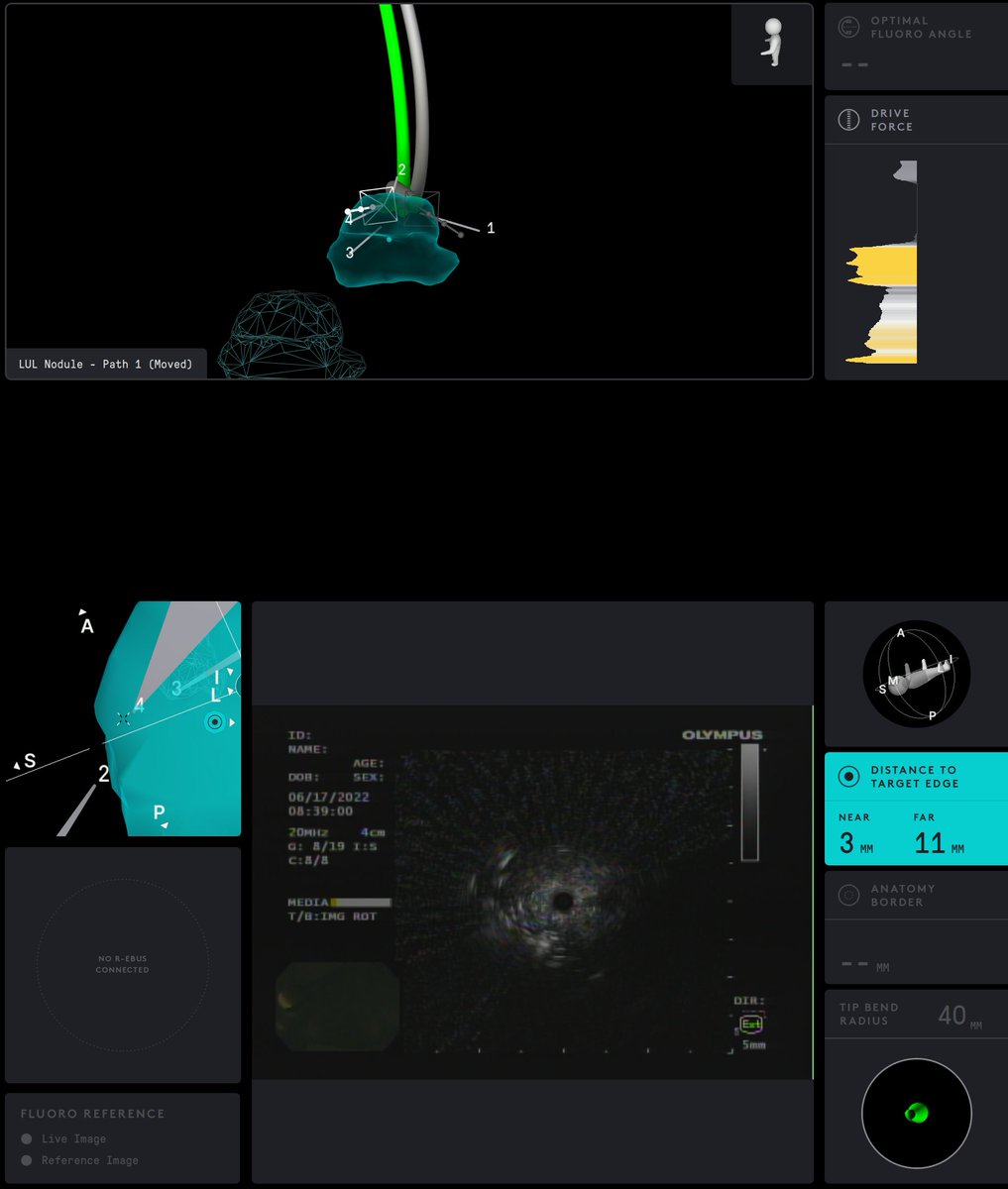
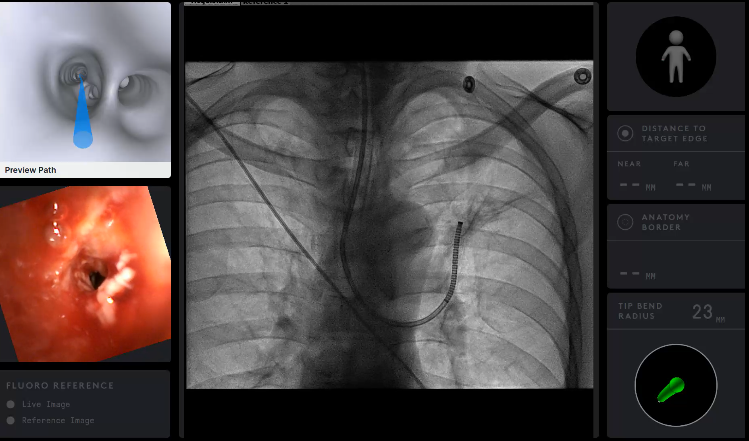
Growing LUL pleural based lesion with no airway leading to it and negative on IR biopsy. Was able to navigate close (within 2cm) to the lesion, biopsy, and adjust using CBCT. Positive for poorly differentiated carcinoma. I would have never tried this without CBCT and Robotics.
I used pulmonary forceps to dilate as I did not have any other dilation tools at my disposal that would fit through the robot (>100cm and <2.0mm). Would love to hear of other ideas/tools to better fix this problem in the future.
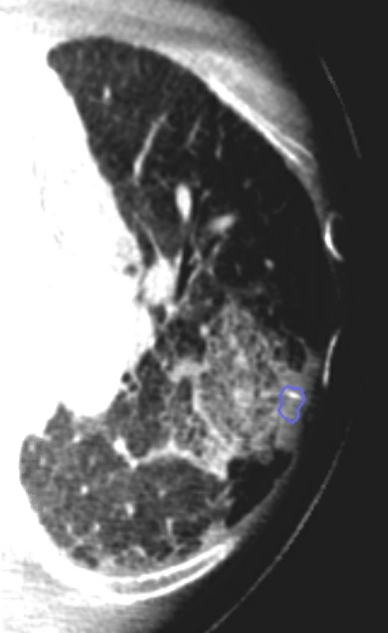
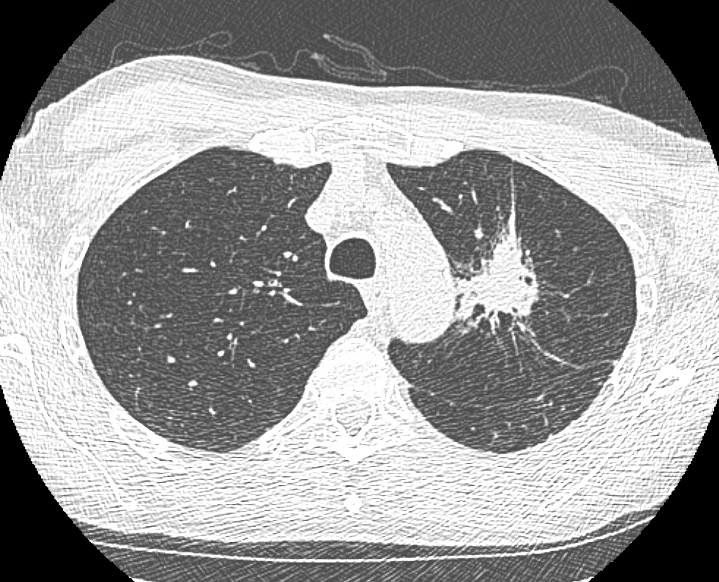
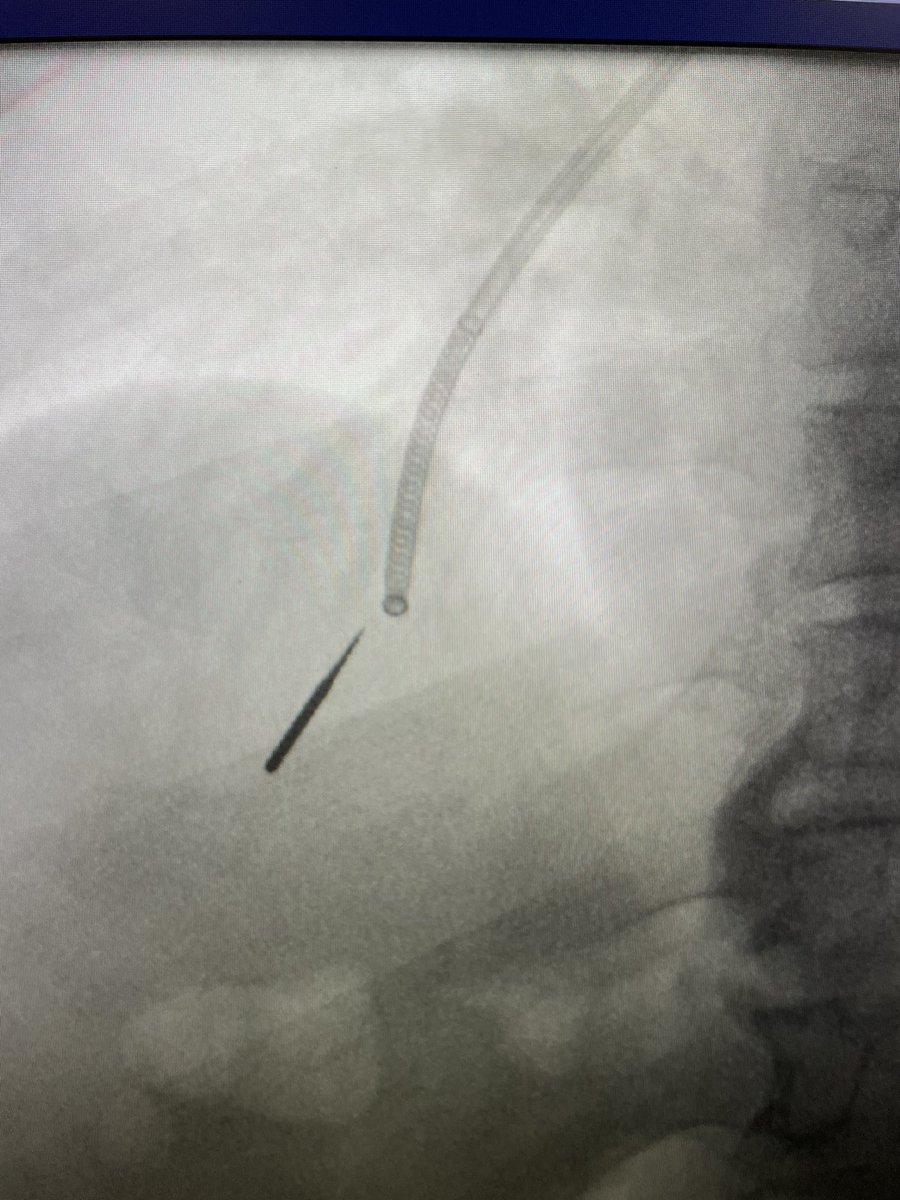
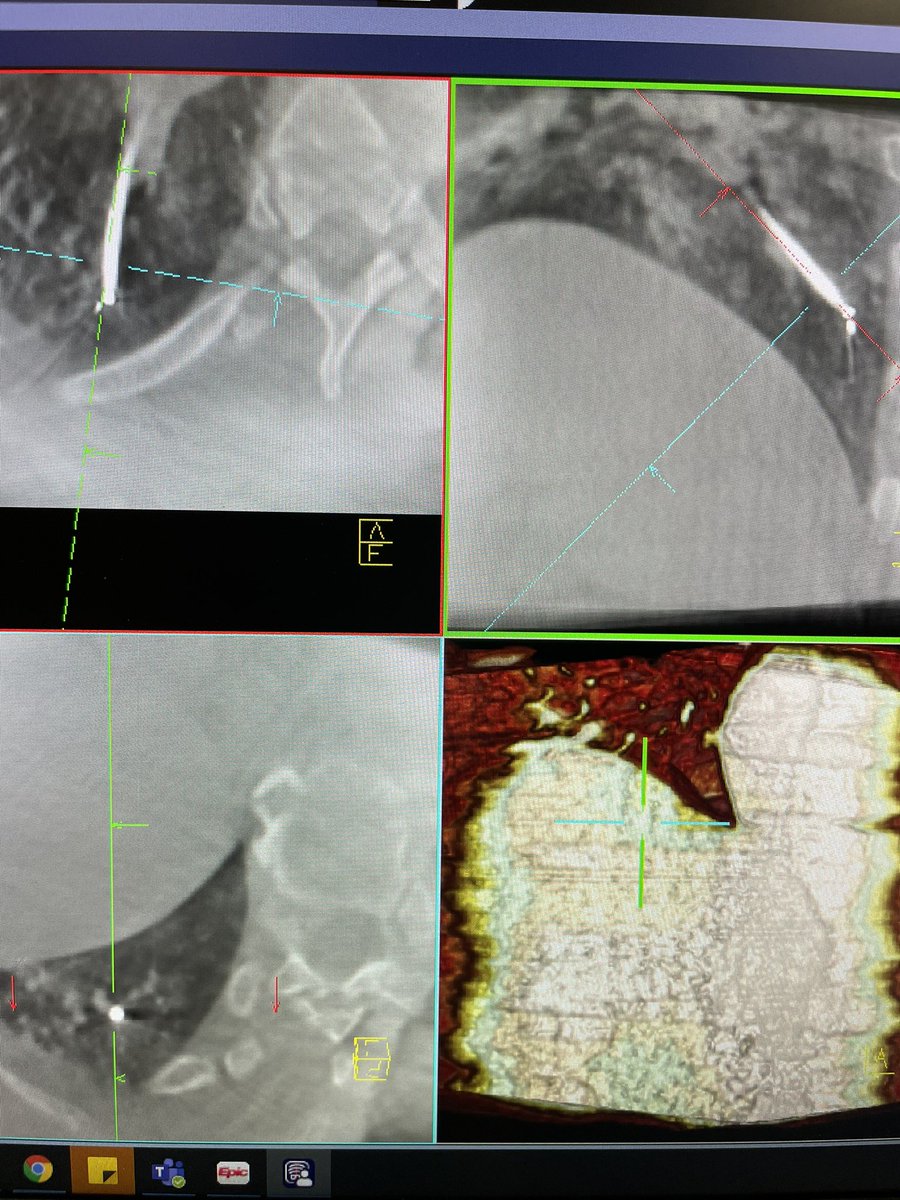
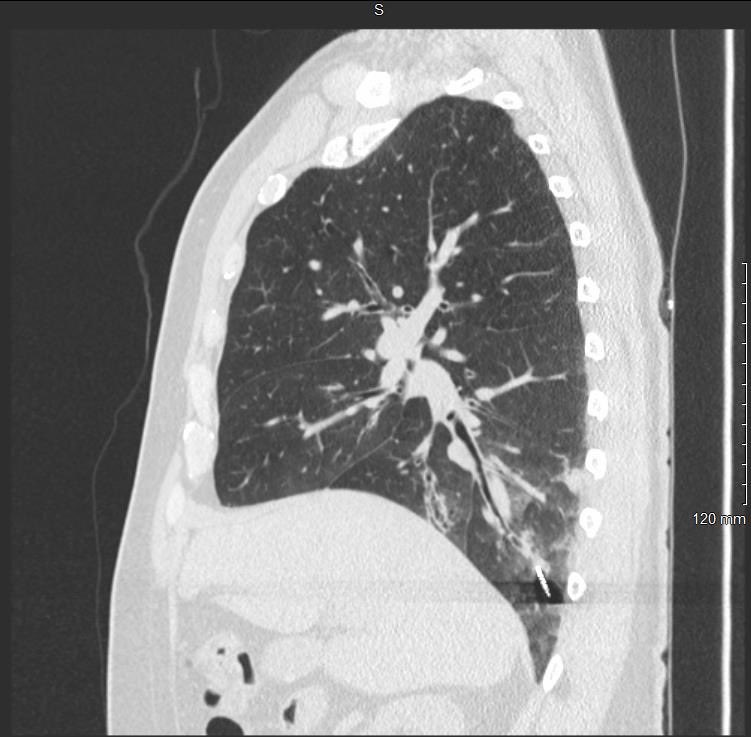
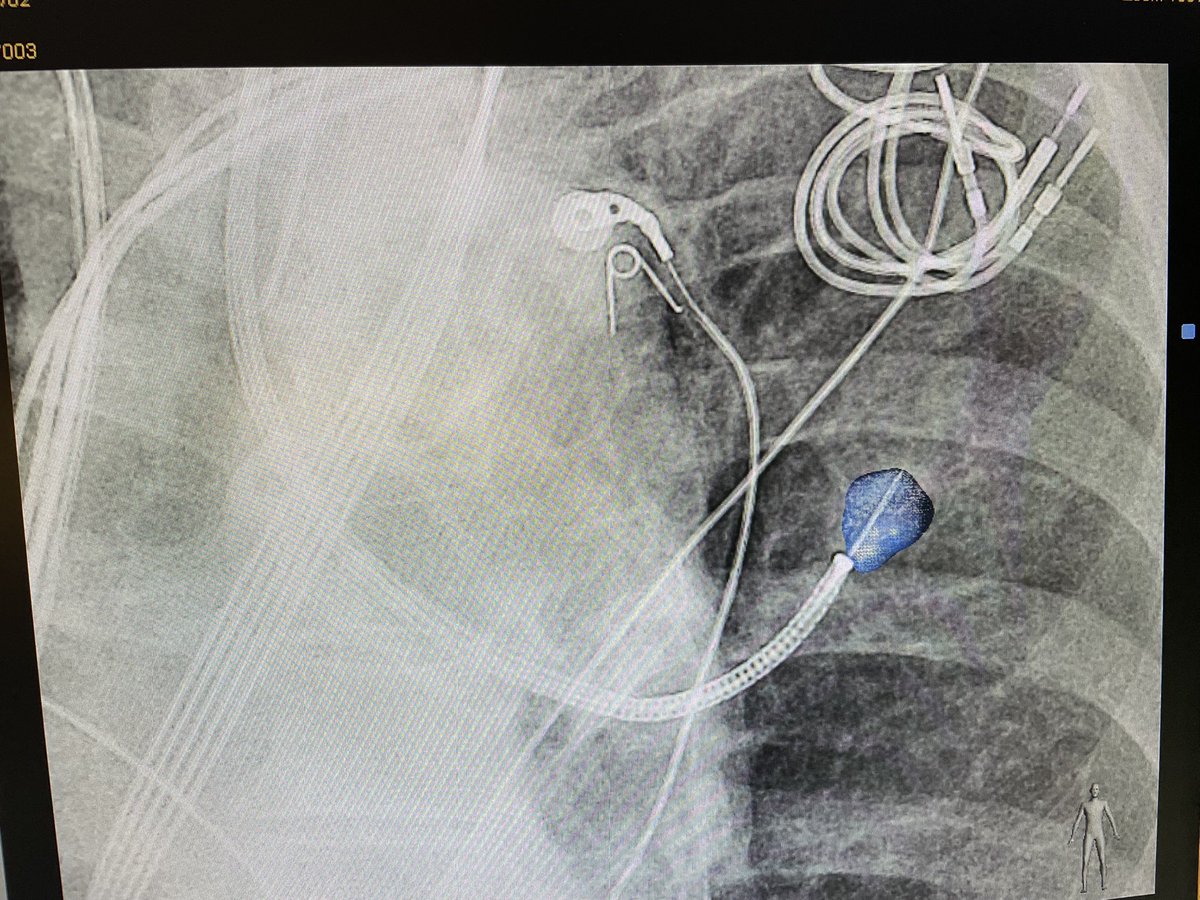
A (useful?) workaround: This patient had radiation to a LUL lesion (First image). Another more apical PET-avid lesion arises, but to get to the apical lesion I had to go through the radiated area. I found the airway was very dense and severely stenosed (Second image).
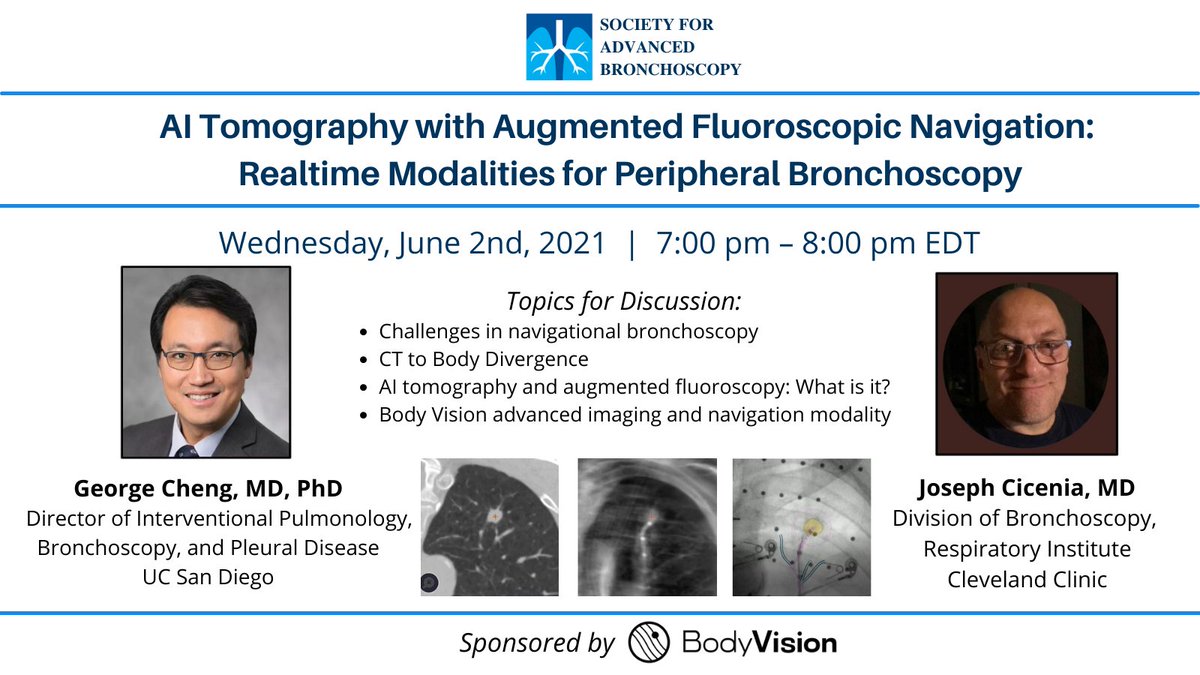
TONIGHT'S LIVE webinar is @ 7pm EST! Hear from Drs. George Cheng and Joseph Cicenia as they discuss challenges in navigational bronchoscopy, CT to body divergence & more! tinyurl.com/y8kjjrv9
REGISTER TODAY for our 2021 SAB SUMMIT-Virtual Conference on Saturday, June 12th from 7:30am-3:00pm. Hear from Drs. Rajani Surendar Bhat & Tom Gildea as they discuss "Palliative Care and Advanced Bronchoscopy" REGISTER HERE>>tinyurl.com/5c2xj6n2#Educate#Innovate#Empowe
89% patients developed atelectasis in at least 1 out of 8 segments and 72% patients in at least 4 segments during bronchoscopy under general anesthesia: hubs.ly/H0D8cKG0#journalCHEST