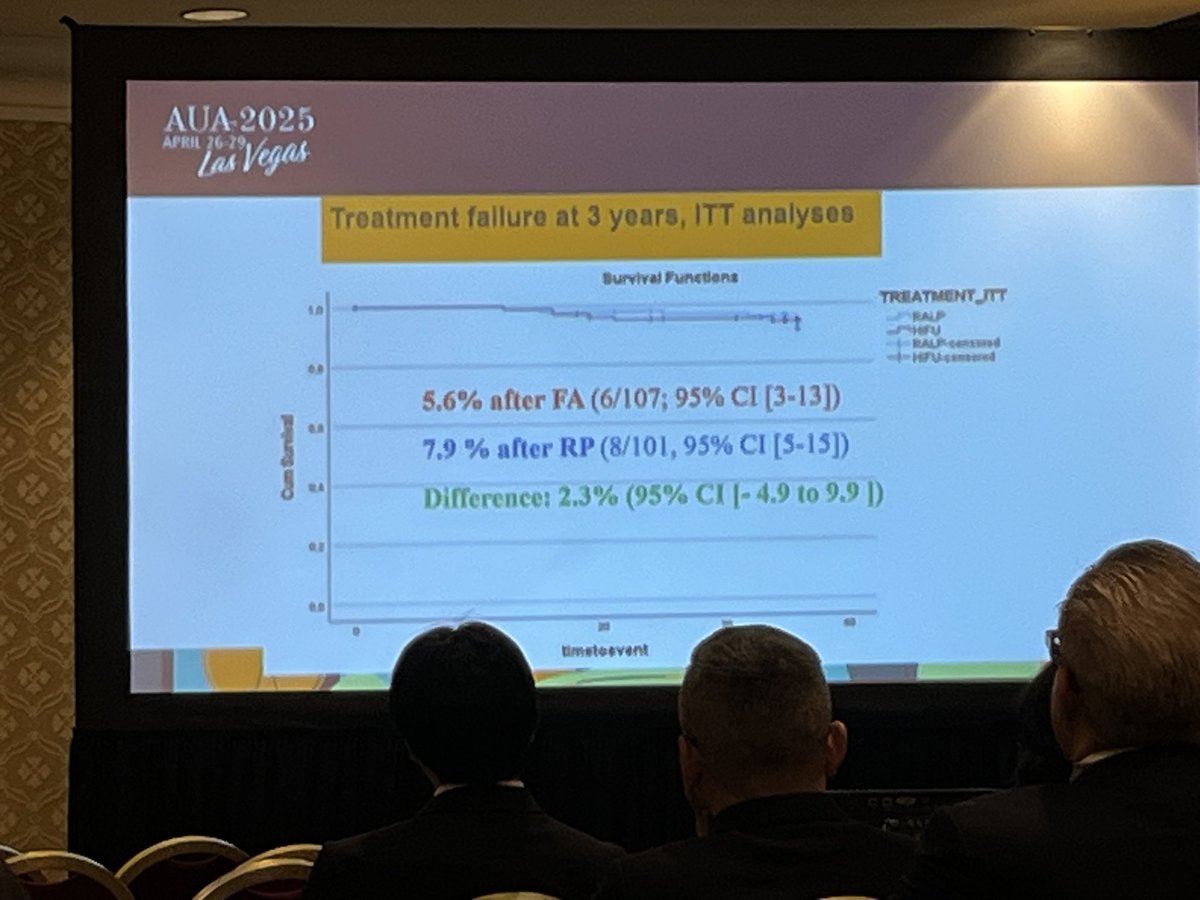
Any KM curve showing biopsy results from AS or focal therapy should include, on the same graph a freedom from biopsy KM curve! It’s hard to interpret without knowing the denominator. #eau26 #prostatecancer
English
John Rewcastle, PhD
668 posts

@rewcastle_john
Not a urologist but I study urology: prostate cancer screening, biopsy, treatment & harm reduction. Also dabble in regulatory affairs. Opinions are my own.


Fantastic Masterclass in Robotic HIFU today at @CleClinicUro London @FocalOneHIFU Thank you to @FocalOneHIFU @SNathanUK for inviting me Lots to think about- starting focal therapy service, advantages of robotic platform, patient selection, guidelines, contemporary trial data…