Autoimmune hepatitis is not just “positive antibodies”—the real clue is persistent hepatocellular inflammation with raised IgG after excluding common mimics.
Like, share & follow for more high-yield clinical pearls.
#AutoimmuneHepatitis#Hepatology#InternalMedicine#MedEd
𝗙𝗲𝗹𝘁𝘆'𝘀 𝘀𝘆𝗻𝗱𝗿𝗼𝗺𝗲
◦ The classic triad of seropositive rheumatoid arthritis (RA), persistent neutropenia (<2,000/mm3), and splenomegaly of varying size (ranging from subclinical, only detectable by imaging tests, to massive) is characteristic of Felty's syndrome (FS), described in 1924 by the American physician Augustus R. Felty.
◦ FS is a rare systemic complication of RA that occurs in less than 1% of cases, primarily those of long duration, with severe joint involvement and extra-articular manifestations, and a strong association with the HLA-DR4 haplotype (almost 95% of cases).
◦ Splenomegaly is not a mandatory feature for the diagnosis of FS and spleen size does not correlate to the severity of RA or neutropenia. Anemia and thrombocytopenia may also be present.
◦ Large granular lymphocyte (LGL) expansion is observed in 30–40% of patients with FS. When LGL expansion is monoclonal and associated with infiltration of the bone marrow and spleen by these cells, the condition is called LGL leukemia, a chronic low-grade lymphoproliferative disorder whose clinical presentation is similar to FS. LGL leukemia shows an increased susceptibility to bacterial infections associated with neutropenia, anemia and splenomegaly, which is why it has also been called "pseudo-Felty".
📊 Comparison of Large Lymphocyte Leukemia associated with Rheumatoid Arthritis (pseudo-Felty) and Felty's Syndrome.
From: Medlin, J., Ishizawar, R.C. (2019). Felty’s Syndrome. In: Tarrant, T. (eds) Rare Rheumatic Diseases of Immunologic Dysregulation. Rare Rheumatic Diseases. Springer, Cham.
Insulin resistance is often reduced to “high glucose”. But that is only the surface of the problem.
Insulin is not simply a hormone that lowers blood sugar.
It is a systemic anabolic signal.
After a meal, insulin tells the body that nutrients are available and that energy can be stored, used, or redirected.
In skeletal muscle, insulin promotes glucose uptake through GLUT4 translocation.
This is one of its most familiar actions: glucose leaves the bloodstream and enters muscle fibres, where it can be oxidised or stored as glycogen.
In the liver, insulin suppresses glucose production.
It inhibits gluconeogenesis and glycogen breakdown, while favouring glycogen synthesis. In other words, after eating, the liver should stop behaving as if the body were fasting.
In adipose tissue, insulin inhibits lipolysis.
It tells fat cells not to release fatty acids into the circulation, because energy is already abundant. At the same time, it favours lipid storage.
But insulin also regulates protein metabolism, vascular tone, mitochondrial function, inflammation, and cellular growth pathways. It is not a “glucose hormone”; it is a metabolic coordinator.
Insulin resistance appears when tissues no longer respond adequately to that signal.
The pancreas compensates by secreting more insulin, often for years. This creates a paradox: insulin levels are high, but insulin action is incomplete.
The consequence is not uniform failure.
Some insulin pathways become resistant, while others remain active. Glucose uptake in muscle may fall, and hepatic glucose production may remain inappropriately high. Yet lipogenesis in the liver can continue, contributing to fatty liver and hypertriglyceridaemia.
Meanwhile, adipose tissue releases more fatty acids, feeding hepatic fat accumulation and interfering with insulin signalling in muscle and liver. Chronic low-grade inflammation, ectopic lipid deposition, mitochondrial stress, and adipokine imbalance amplify the loop.
This is why insulin resistance is not just a prelude to type 2 diabetes. It is a whole-body disorder of nutrient partitioning.
Insulin resistance means that the body hears abundance, but its tissues behave as if the message were distorted. The problem is not only excess sugar in blood, but a loss of metabolic synchrony.
🚨 معظم مرضى السكري يستهدفون رقم واحد فقط.. لكن توصيات جمعية السكر الأمريكية 2026 تقول: الهدف يختلف من شخص لآخر (ويقلل المضاعفات بنسبة كبيرة لو طبقناه صح)
📊 للمرضى:
🔹 مخزون السكر التراكمي HbA1c: أقل من 7%
🔹 سكر قبل الأكل: 80-130 مجم/ديسيلتر
🔹 سكر بعد الأكل بساعتين: أقل من 180
🔹 باستخدام مجس قياس السكر: Time in Range (70-180) أكثر من 70%
📍 للأطباء (التفاصيل الدقيقة):
- هدف أقل (<6.5%) → للمريض اللي على المنظمات، خطر هبوط سكر منخفض
- هدف أعلى (<8%) → كبار السن أو مع أمراض معقدة أو ضعف وظيفي أو خطر هبوط عالي
- دائماً: إعادة تقييم الهدف كل زيارة + مشاركة المريض في القرار
- إذا TIR <70% أو TBR >4% → غيّر أو خفّف العلاج فورا
(هذا الجدول عشان ترجع له في أي زيارة )
❤️ HOW BLOOD ACTUALLY FLOWS THROUGH THE HUMAN HEART ❤️
The heart is essentially a two-sided pump with one simple rule:
🔵 Right side = Deoxygenated blood → Lungs
🔴 Left side = Oxygenated blood → Body
Master that concept and the entire circulation becomes easy.
🫀 BLOOD FLOW PATH
1️⃣ Body → Right Atrium
Deoxygenated blood returns via:
• Superior Vena Cava (upper body)
• Inferior Vena Cava (lower body)
⬇️
2️⃣ Right Atrium → Right Ventricle
Through the Tricuspid Valve
⬇️
3️⃣ Right Ventricle → Lungs
Through the Pulmonary Valve into the Pulmonary Artery
📌 High-yield:
The Pulmonary Artery is the ONLY artery carrying deoxygenated blood.
🌬️ LUNGS
At the alveoli:
❌ CO₂ leaves
✅ O₂ enters
Blood becomes oxygen-rich.
⬇️
4️⃣ Lungs → Left Atrium
Via the Pulmonary Veins
📌 High-yield:
The Pulmonary Veins are the ONLY veins carrying oxygenated blood.
⬇️
5️⃣ Left Atrium → Left Ventricle
Through the Mitral (Bicuspid) Valve
💪 The Left Ventricle has the thickest myocardium because it must pump blood throughout the entire body.
⬇️
6️⃣ Left Ventricle → Aorta
Through the Aortic Valve
🚀 Oxygenated blood is delivered to every organ and tissue.
⬇️
7️⃣ Capillaries
Oxygen and nutrients are delivered.
Carbon dioxide and metabolic waste are collected.
⬇️
8️⃣ Veins → Vena Cava → Right Atrium
🔄 The cycle repeats continuously.
🩺 THE FOUR HEART VALVES
➡️ Tricuspid:
Right Atrium → Right Ventricle
➡️ Pulmonary:
Right Ventricle → Pulmonary Artery
➡️ Mitral:
Left Atrium → Left Ventricle
➡️ Aortic:
Left Ventricle → Aorta
🧠 Memory Hack:
"Try Pulling My Aorta"
T = Tricuspid
P = Pulmonary
M = Mitral
A = Aortic
❤️ Your heart performs this complete circuit roughly 100,000 times every day without a single conscious thought.
Absolutely remarkable.
#Cardiology#MedEd#FOAMed#MedicalEducation#Anatomy#Physiology#Heart#MedTwitter
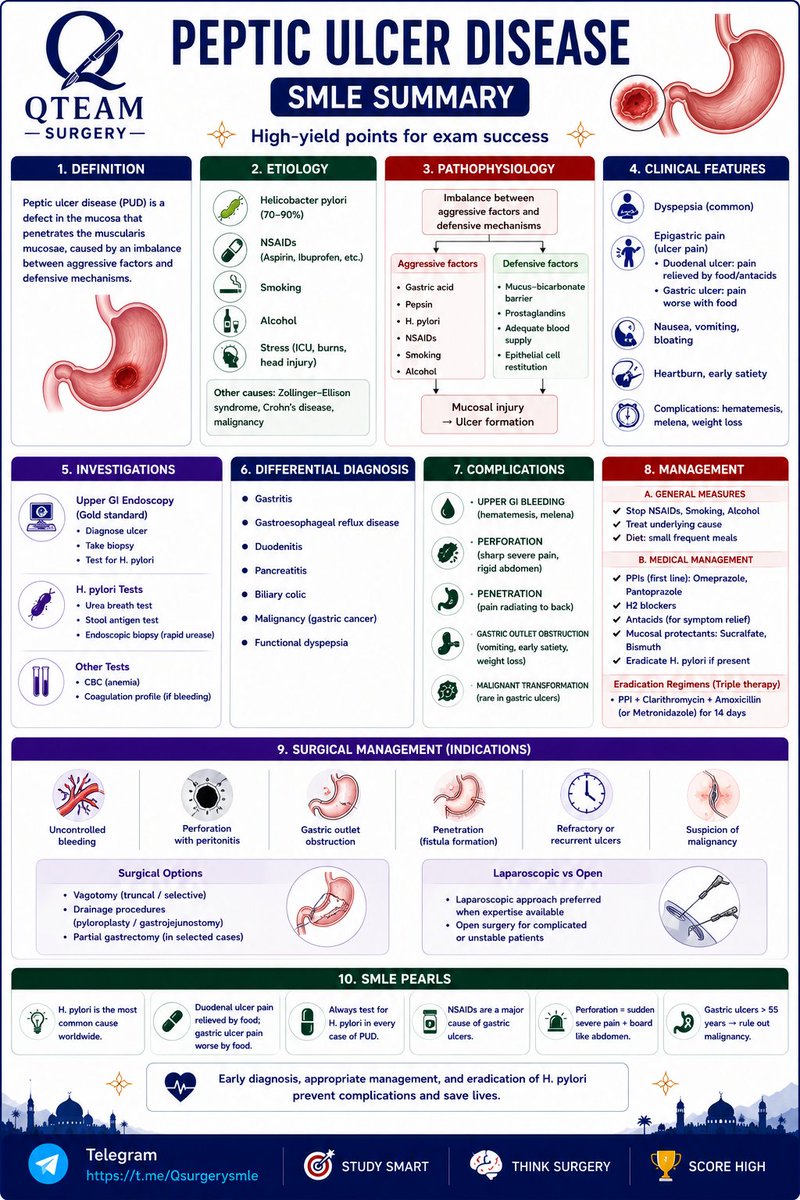
🚨 PEPTIC ULCER DISEASE — SMLE SUMMARY
A classic topic that appears in both surgery and internal medicine exams 🩺
This visual summary covers:
▫️H. pylori and NSAIDs as the major causes
▫️Gastric vs duodenal ulcer differences
▫️Clinical presentation and red flags
▫️Diagnostic approach and endoscopy findings
▫️Medical management and H. pylori eradication
▫️Complications: bleeding, perforation, penetration, obstruction
▫️When surgery is indicated
▫️High-yield SMLE pearls for quick revision
Master the complications and you'll solve most PUD questions with confidence 🔥
Telegram: t.me/Qsurgerysmle
Which contraceptive has the highest typical use failure rate?
(A) Levonorgestrel IUD
(B) Combined oral contraceptive pill
(C) Male condom
(D) Subdermal implant
#MCQ
∆ The Johnson Maneuver- It is an emergency obstetric procedure used for the manual replacement of an acute postpartum uterine inversion.
• The clinician places their hand inside the vagina, cups the inverted fundus, and pushes it along the pelvic axis back into the abdominal cavity.
• Once replaced, the hand is held as a fist inside the cavity to maintain structure while uterotonics are given to prevent re-inversion.
• This critical intervention is performed immediately to prevent life threatening postpartum hemorrhage and profound neurogenic or hypovolemic shock.
It's Johnson's Maneuver.
Indication:- Acute puerperal uterine inversion (usually after delivery).
Technique:-
The inverted uterine fundus is pushed upward through the cervix toward its normal anatomical position using the palm and fingers.
This is the first-line manual method for immediate correction of uterine inversion.
Key Point:-
Umbilical cord prolapse - Johnson's maneuver = elevate presenting fetal part.
Uterine inversion - Johnson's maneuver = manually reposition the inverted uterus.
Uterine prolapse - No specific "Johnson's maneuver"; management involves pelvic floor exercises, pessary, or surgery depending on severity.
D. Talus.
• It is unique among tarsal bones for having no muscular or tendinous attachments.
• It relies entirely on ligamentous support and surrounding bony structures for its stability within the ankle joint.
• In contrast, the scaphoid, pisiform, and patella all serve as functional attachment sites for specific muscles or tendons.