
Ernest Spitzer
225 posts

Ernest Spitzer
@spitzertweets
#cardiology #clinicaltrials #leadership #innovation #evolution #thefutureisnow #warpjump (opinions are personal)
The Netherlands Katılım Nisan 2022
102 Takip Edilen131 Takipçiler

My thoughts on IVUS-CHIP & OPTIMAL
Yes, I'm also still digesting the results from IVUS-CHIP and OPTIMAL. I think we all are. And I understand why we as a community are having some trouble sitting with these results.
But first, I have to disclose my conflicts of interest: I'm a proctor and speaker for Boston Scientific, specifically for CHIP interventions. I've been doing this for years. So yes, I have skin in this game too, and these results challenge some of my own deeply held beliefs about how we do interventional cardiology. That's exactly why I think we owe it to ourselves to think clearly here, not defensively.
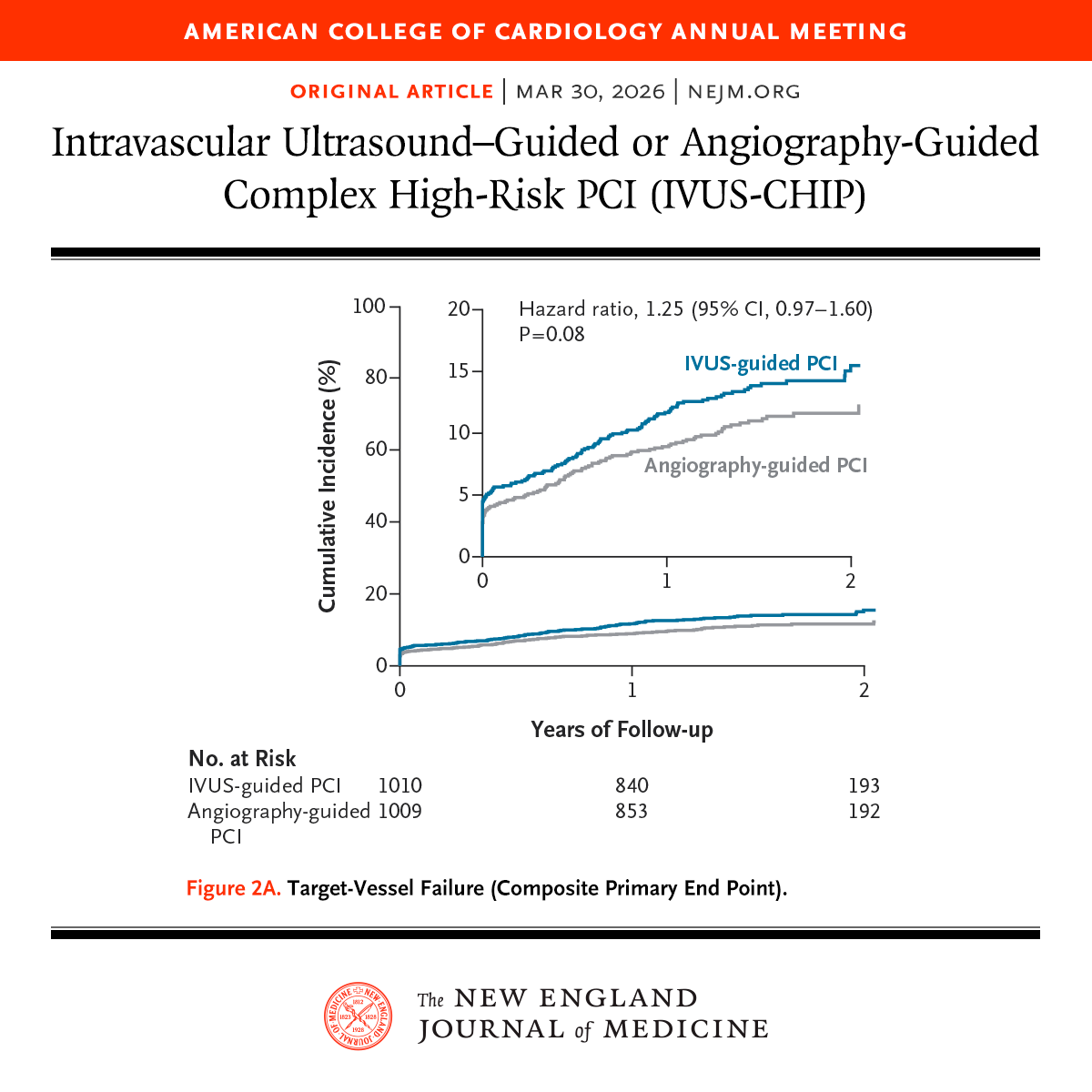
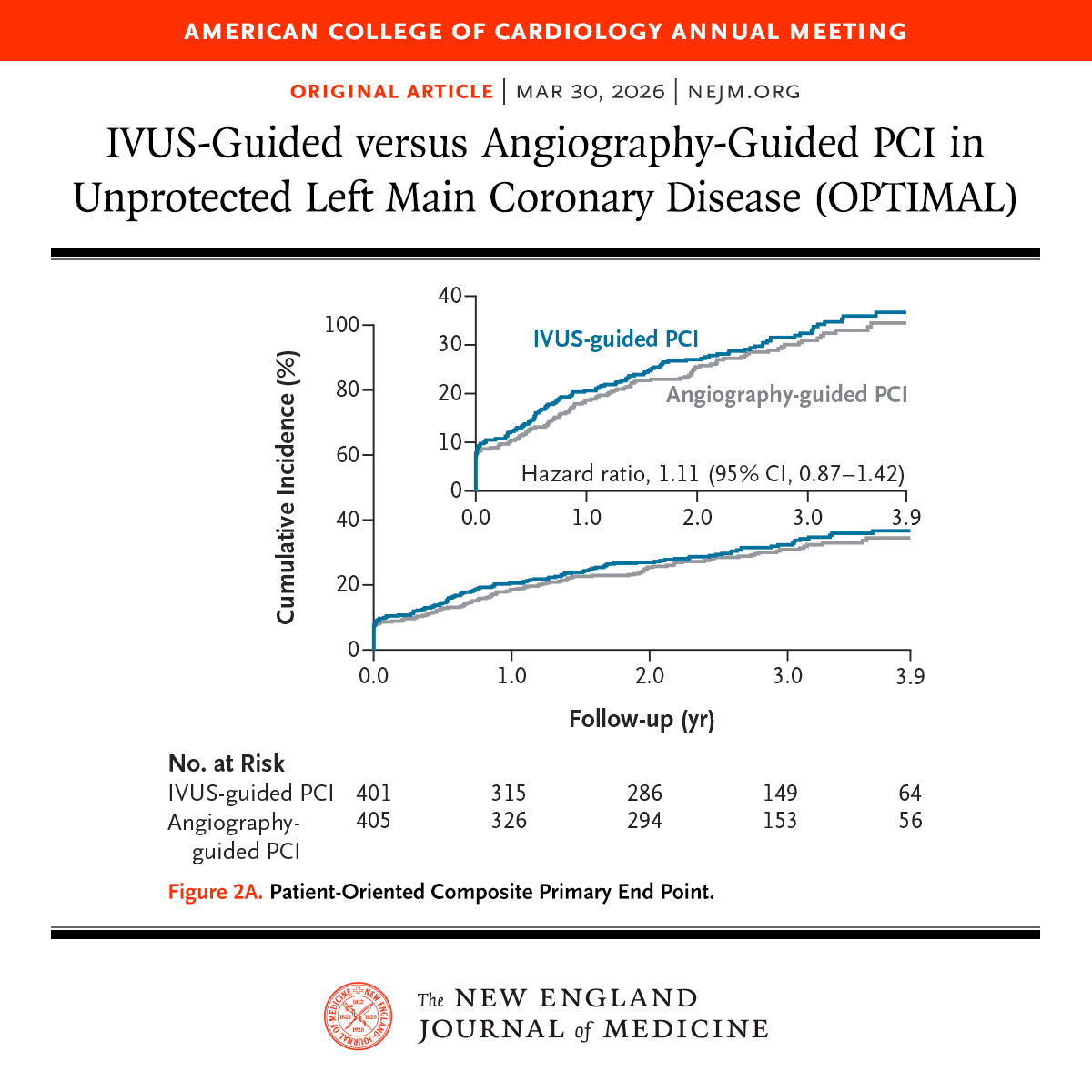
So let's look at what happened. IVUS-CHIP: HR 1.25 (0.97–1.60). OPTIMAL: HR 1.11 (0.87–1.42). Two large, well-designed European trials, both published simultaneously in NEJM, both neutral — and both trending numerically against IVUS. That stings. I get it.
But here's what's been bothering me about the reaction. The most common defense I keep seeing is: "IVUS-CHIP failed because only 48% of lesions met the predefined optimization criteria." And I understand the instinct — if the intervention wasn't properly delivered, how can we judge it? Fair enough. But let's check the receipts.
ULTIMATE — the trial we all love to cite as proof that IVUS works — achieved optimization in 53%. RENOVATE — arguably the strongest positive IVUS trial we have — achieved ~58%. OCTIVUS — 55% in the IVUS arm. IVUS-CHIP: 48%.
Do you see the problem? The difference is marginal, but the way we treat these numbers is completely asymmetric. We celebrate ULTIMATE at 53% as a win for IVUS. We dismiss IVUS-CHIP at 48% as a flawed trial. That's not consistent. Either suboptimal implementation invalidates all of these trials, or it invalidates none of them. We have to pick one.
And honestly, I think the real answer is simpler than we want it to be. Maybe 50–55% optimization isn't a failure of any particular trial. Maybe it's a biological ceiling. Diffuse disease, heavy calcium, tortuous anatomy — there are lesions where clean landing zones simply don't exist, no matter how good the operator or the imaging. Look at the substrates: IVUS-CHIP had 45.8% severe calcification and a mean distal edge plaque burden of 47.6% — nearly failing the optimization criterion by definition. RENOVATE had 13.5% severe calcification and 40.6% distal plaque burden. Same tool, same criteria, vastly different biology. We can't keep blaming the operator when the anatomy won't cooperate.
And this leads to an uncomfortable thought: maybe reaching stent optimization criteria says more about the anatomy you're working with than the technique you're using. We can achieve what the vessel allows us to achieve — nothing more. Better anatomy = higher optimization rates = better outcomes. That's not IVUS working better. That's easier disease behaving better. And if that's true, then the positive trials may have been telling us more about their patient population than about the tool itself.
There's another criticism that deserves pushback: "In OPTIMAL, operators only acted on IVUS findings in about 30% of cases — so IVUS wasn't really used." But let's be fair here. A diagnostic tool can't do anything by itself. It depends entirely on how we react to what it shows us. And saying that operators "didn't act" in 70% of cases assumes there was something to act on. We don't actually know that. Maybe the result was already good. Maybe the IVUS confirmed what the operator had already achieved by angiography alone. And if that's the case, it doesn't indict the tool or the trial — it tells you something important about operator quality. These weren't operators ignoring IVUS. These were operators who were already so good that IVUS had nothing left to add.
Now, here's the part that I think nobody really wants to say out loud: maybe IVUS already won. Not by proving superiority in a trial — but by making us better operators over the past decade.
Look at the post-dilation rates in the angiography arm across the major IVUS trials: ULTIMATE 57%, RENOVATE 75%, IVUS-CHIP 84.5%, OPTIMAL 96%. Look at that progression. Operators who've used IVUS routinely for years have internalized everything it taught them — sizing, post-dilation, POT, landing zone selection. When they get randomized to the angiography arm, they turn off the screen, but they don't turn off the IVUS-calibrated brain. POT in 85% of cases. Systematic post-dilation. Aggressive sizing. The control arm in these trials isn't naive angiography. It's IVUS without IVUS.
So the real comparison isn't imaging vs no imaging. It's formal IVUS vs the knowledge that IVUS has already embedded into how we practice. And when the gap between those two narrows to nothing, the incremental benefit of the screen disappears. That's not a failure. If anything, that's graduation.
To be clear: this does NOT mean IVUS is useless, and it certainly doesn't mean you should stop using it. What it does mean is that in expert European centers — with operators who've spent years calibrating their eyes with imaging — the marginal gain of formal IVUS guidance over their IVUS-informed angiography is effectively zero.
One thing I'd genuinely like to see from both trials: the same analysis ULTIMATE did — outcomes in patients who actually achieved optimization criteria vs those who didn't. In ULTIMATE, that landmark analysis showed TVF of 4.2% vs 9.2% (HR 0.44). That was the strongest argument we had that when IVUS-guided optimization is truly achieved, it works. If IVUS-CHIP and OPTIMAL show the same pattern, the conversation changes entirely: the problem isn't IVUS — it's that we can't implement it fully in half the patients. And if they don't show that pattern, we need to accept that too.
But here's the pill I think we all need to swallow, myself included: we can't keep invoking "optimization failure" only when results disappoint us. 53% in ULTIMATE = proof IVUS works. 48% in IVUS-CHIP = proof the trial was flawed. That's not how science works. That's narrative fitting. And we're better than that.
#CardiologyX #IVUS #PCI #OPTIMAL #CHIPIVUS #ACC26
English

@spitzertweets @mmamas1973 The trial tells us expert hands can approximate it. It doesn’t tell us angiography alone is sufficient everywhere.
Sorry about the long response 😁
English
🧵So OPTIMAL just dropped at ACC.26, and I’ll be honest — it’s going to make a lot of interventionalists very UNCOMFORTABLE.
806 patients 😮. Unprotected left main PCI. Randomized to IVUS vs angiography guidance.
Result? No difference.🤯

English
These data are difficult to digest and are nuanced. Assuming that some of the largest centers in Europe and top-performing imagers (looking at the co-authors) did not use IVUS information appears as looking things upside down. A better look is that expert operators recalibrated their angio-only practices with IVUS knowledge making the impact (i.e., effect size) smaller or non-existent. Stent thromboses were much lower in IVUS CHIP, though. Education and training are key and the adequate learning-curve volumes are unknown.
English
My cynical read: IVUS works when you actually USE the information it gives you. A probe in the artery operated by someone who ignores it is just an expensive catheter.
The question was never “IVUS vs angiography.” It was always “good operator vs bad operator.”
Uncomfortable? 😳
English
@mmamas1973 @mirvatalasnag @djc795 @twj1974 @nicolasamabile @NievesGonzalo1 @DrNataliaP @SripalBangalore Done ✅ Looking forward 🤝
English

@spitzertweets @mirvatalasnag @djc795 @twj1974 @nicolasamabile @NievesGonzalo1 @DrNataliaP @SripalBangalore If you follow me back we can take this via messages 👍
English

How do we reconcile these results with other trials like IVUS XPL & RENOVATE Complex PCI?
@djc795 @twj1974 @mmamas1973 @nicolasamabile @NievesGonzalo1 @DrNataliaP @SripalBangalore
NEJM@NEJM
Presented at #ACC26: In the IVUS-CHIP trial involving patients undergoing complex high-risk PCI, the risk of target-vessel failure (a composite outcome) was not lower with intravascular ultrasound guidance than with angiography guidance. Full trial results: nejm.org/doi/full/10.10… Editorial: IVUS — A Zigzag Path to Success nejm.org/doi/full/10.10… @ACCinTouch
English
@mmamas1973 @mirvatalasnag @djc795 @twj1974 @nicolasamabile @NievesGonzalo1 @DrNataliaP @SripalBangalore Happy to discuss how to make it happen 🤝
English
@spitzertweets @mirvatalasnag @djc795 @twj1974 @nicolasamabile @NievesGonzalo1 @DrNataliaP @SripalBangalore there have been several studies that have validated our score- but as yet no prospective study using this score to study an intervention
English
@mmamas1973 @mirvatalasnag @djc795 @twj1974 @nicolasamabile @NievesGonzalo1 @DrNataliaP @SripalBangalore This is indeed an interesting approach. Curious about prospective studies using this score 👍
English
I actually think in relation to my own study if I was designing it again I would define complex PCI differently. I don't think individual components of complexity are useful. I would personally use a validated risk score like our bcis chip score- and define complexity as a risk of greater than 5% in patient mortality which equates to top 5% highest risk cases
➡️ jacc.org/doi/10.1016/j.…
English
@mmamas1973 @mirvatalasnag @djc795 @twj1974 @nicolasamabile @NievesGonzalo1 @DrNataliaP @SripalBangalore If we look at the frequency of CTOs (approx 20%), heavy calcification (approx 45%), and SYNTAX score of 25, I wouldn’t conclude that IVUS-CHIP had simple, direct-stented long lesions as the most frequent type, but this is a great consideration to be explored further.
English
@spitzertweets @mirvatalasnag @djc795 @twj1974 @nicolasamabile @NievesGonzalo1 @DrNataliaP @SripalBangalore In relation to 28 mm, we all agree that these typeset of lesions are at slightly increased risk, but absolute risk remains low. I think most people wouldn't class a lesion that they have directly stented with a 30 mm stent as a chip case!
English
That is correct. Not all bifurcations require a 2 stent approach, consequently, this was not mandatory. And in relation to heavy calcification the numbers speak for themselves in the supplement. We see approx. 45% in IVUS-CHIP vs. <20% in RENOVATE. Penetration of IVL remains low and needs further education (and data as well).
English
When the video comes out you can watch it where the PI confirmed that bifurcations did not require a 2 stent approach to be enrolled. In relation to calcification I think that if only a minority of cases require calcium modification then that isn't heavy calcification- your opinion may of course differ
English

OPTIMAL and IVUS-CHIP don’t show imaging is ineffective. They just show how much it has already shaped modern PCI.
The control arms weren’t imaging-naïve, but IVUS-trained operators applying what IVI has already taught them.
Let’s not mistake the ceiling for the floor.
English
No lo llamaría contradicción, sino evolución. Hace 20 años IVUS ayudaba a mejorar las estrategias de ICP. Hoy los algoritmos de ICP son muy similares con o sin imágenes intracoronaria. Predilatación, modificación de lesiones, post-dilatación son ya rutinarios sin imágen intracoronaria. Hemos recalibrado el ICP con angiografía en base al conocimiento del IVUS.
Español

Wow! contradice evidencia previa
NEJM@NEJM
Presented at #ACC26: Among patients with unprotected left main coronary artery disease, intravascular ultrasonography–guided PCI did not result in a lower risk of ischemic events or death than angiography-guided PCI. Full OPTIMAL trial results: nejm.org/doi/full/10.10… Editorial: Seeing the Left Main Coronary Artery Clearly — Is IVUS Always Necessary? nejm.org/doi/full/10.10… @ACCinTouch
Español
@omendiz Please see our supplements, where we compared Asian, US, and EU studies. Geography matters. EU patients were sickest, highest risk ever reported. All centers high volume (>1000 PCIs /year).
English
Is there a different angiography interpretation from Europe, America and China to explain such contradictory information in this morning ??🤔
NEJM@NEJM
Presented at #ACC26: In the IVUS-CHIP trial involving patients undergoing complex high-risk PCI, the risk of target-vessel failure (a composite outcome) was not lower with intravascular ultrasound guidance than with angiography guidance. Full trial results: nejm.org/doi/full/10.10… Editorial: IVUS — A Zigzag Path to Success nejm.org/doi/full/10.10… @ACCinTouch
English
Our data strongly suggests geographic differences. IVUS-CHIP is the highest risk population ever enrolled (please see our comparative tables in the supplement): older patients, higher prior MI and prior revascularizations, much higher heavy calcification, left main disease, and CTOs compared to prior trials. All high volume, expert centers. Much higher plaque burden at edges despite longer stents. Different geographies, different CAD burden, different practice, different outcomes, and different effect size. Data ought to be reconciled, at least in Europe.
English
Of course and the argument can be misleading without additional info. In IVUS-CHIP, non-complex lesions were to be treated according to the randomized strategy except for concurrent non-complex lesions <2.5 mm in diameter, which were left to the operator. All complex lesions (including those with diameter <2.5 mm) underwent IVUS-guidance. Approx. 12% of the complex (study) lesions were <2.5 mm (similar to RENOVATE COMPLEX PCI) and certainly underwent IVUS-guidance. This is nicely shown in the Supplementary tables. Happy to continue the dialogue after reviewing the Supplement.
English

@mmamas1973 @mirvatalasnag @djc795 @twj1974 @nicolasamabile @NievesGonzalo1 @DrNataliaP @SripalBangalore Is it known why stented lesions <2.5mm in IVUS-CHIP were not IVUS optimized? Was 12% of the stented lesions - and prone to critical underexpansion
English
Highly arguable. Please see our supplement which explains this in detail. IVUS-CHIP has the most complex population ever enrolled in these trials. Heavy calcification (using similar definitions) several X higher than RENOVATE or ILUMIEN Complex or OCTOBER. Prior MI or prior PCI higher as well. We haven’t reported stenting strategies in bifurcations so conclusions cannot be established. Curious why Dr. Mamas suggests that a long lesion is not a complex lesion - all prior meta-analysis on imaging guidance included long lesions as a criterion - some > 20 mm. IVUS-CHIP uses 28+ (recognized cut-off). Robust data that takes some time to digest.
English
@mirvatalasnag @djc795 @twj1974 @nicolasamabile @NievesGonzalo1 @DrNataliaP @SripalBangalore One of the issues is that the complexity of these cases wasn't actually that complex - calcification was defined angiographically I'm very few % of cases need ca modification- bifurcations were mainly single stent lesions and 28 mm not really a major crierion of chip .....
English
Ernest Spitzer retweetledi
My eyes are IVUS crowd wins today 👀!!!
NEJM@NEJM
Presented at #ACC26: Among patients with unprotected left main coronary artery disease, intravascular ultrasonography–guided PCI did not result in a lower risk of ischemic events or death than angiography-guided PCI. Full OPTIMAL trial results: nejm.org/doi/full/10.10… Editorial: Seeing the Left Main Coronary Artery Clearly — Is IVUS Always Necessary? nejm.org/doi/full/10.10… @ACCinTouch
English
Ernest Spitzer retweetledi
Dr. Roberto Diletti and Dr. C. Michael Gibson discuss the IVUS-CHIP trial: IVUS-guided PCI showed similar rates of target vessel failure compared to angio-guided approach among patients undergoing complex high-risk indicated procedures. #ACC26 Watch video here: clinicaltrialresults.org/dr-roberto-dil…
English
Ernest Spitzer retweetledi

Presented at #ACC26:
In the IVUS-CHIP trial involving patients undergoing complex high-risk PCI, the risk of target-vessel failure (a composite outcome) was not lower with intravascular ultrasound guidance than with angiography guidance. Full trial results: nejm.org/doi/full/10.10…
Editorial: IVUS — A Zigzag Path to Success nejm.org/doi/full/10.10…
@ACCinTouch
English
Ernest Spitzer retweetledi
Presented at #ACC26:
Among patients with unprotected left main coronary artery disease, intravascular ultrasonography–guided PCI did not result in a lower risk of ischemic events or death than angiography-guided PCI. Full OPTIMAL trial results: nejm.org/doi/full/10.10…
Editorial: Seeing the Left Main Coronary Artery Clearly — Is IVUS Always Necessary? nejm.org/doi/full/10.10…
@ACCinTouch
English
Not quite. It is time to accept that regional data matters (European practice is not equal to Asian practice and also not equal to US practice - prove me wrong). Moreover, 20+ year-old data no longer represents current practice. Medicine and technical algorithms have evolved, and hazard ratios have narrowed. Nicely shown in our supplements in the NEJM. By the way, ILUMIEN IV was a negative study.
English

@DFCapodanno @CMichaelGibson Since we published our meta-analysis in Lancet there have been 5new major RCTs, these two plus OCCUPI, IVUS-ACS (the largest), and DK CRUSH VIII. These latter three were positive, the two you mentioned negative. An updated meta-analysis would still be markedly positive.
English
Ernest Spitzer retweetledi

OPTIMAL suggests that using IVUS in unprotected left main PCI may cost you 22 minutes with no clinical benefit. One might think it’s an outlier. Yet, the same day, IVUS-CHIP reports no advantage of IVUS over angiography in complex high-risk PCI. Either we have been fundamentally misinterpreting the evidence so far, or we urgently need to reconcile these data. #ACC26
nejm.org/doi/full/10.10…
nejm.org/doi/full/10.10…
English