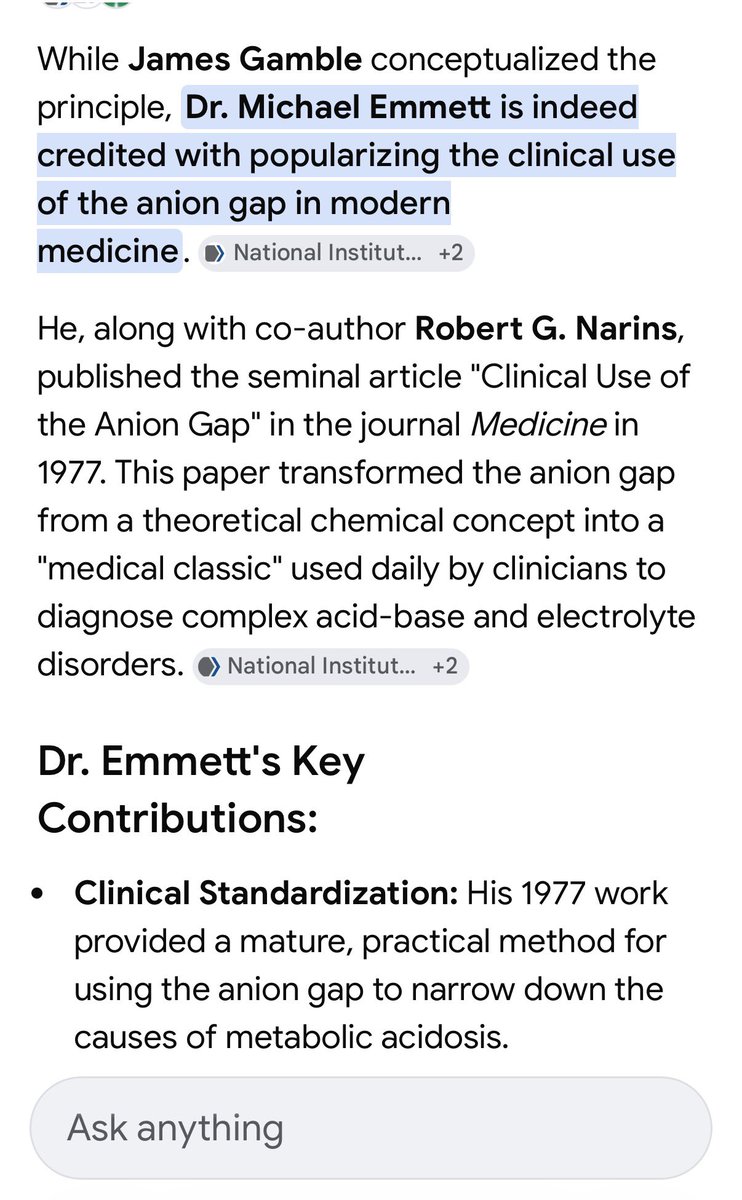
Anyone who has worked with me on inpatient service knows that the Anion Gap is one of my favorite lab tests. So many things it can help diagnose… So imagine how happy I was to meet Dr Emmett, widely credited with popularizing the use of the AG in modern medicine!

English