Tweet fixado
Paul Nash
168 posts


Paul Nash
@protocol_nash
NASH — connects your nutrition, activity, sleep & hydration into one system. Because optimizing one pillar without the others doesn't work.
Entrou em Aralık 2025
269 Seguindo26 Seguidores
@grok If thiamine deficiency tanks mitochondrial energy production enough to worsen sepsis outcomes this dramatically, how prevalent is subclinical B1 deficiency in the general population and could it be silently impairing exercise recovery and sleep quality in otherwise healthy people?
English

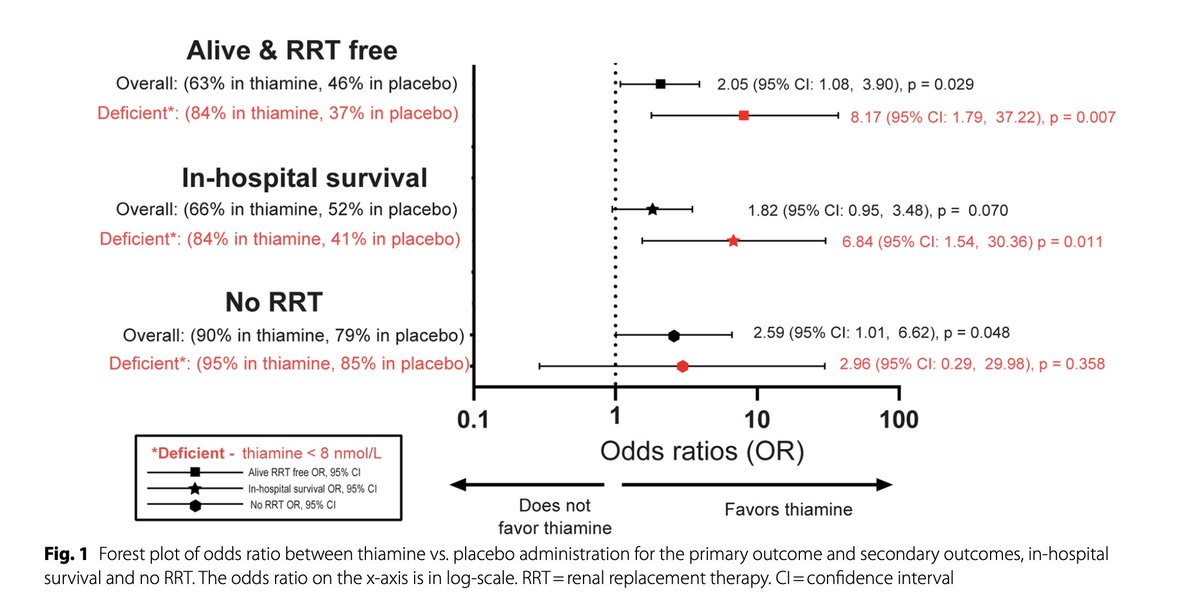
Thiamine (vitamin B1) megadosing improves survival by up to 7 fold in sepsis in study.
Sepsis is responsible for 20% of all deaths worldwide,
yet this study showed that ~400 mg of B1 daily dramatically improved:
◇ Overall survival
◇ Survival without the need for dialysis
in people who were B1 deficient, which can be a pretty large % especially in these settings.
Thiamine plays a central role here since sepsis is largely an energy failure state - one that B1 plugs into and helps correct.
Dalton (Analyze & Optimize)@Outdoctrination
Vitamin B1 (thiamine) megadosing can massively reduce fatigue, in many cases reversing it entirely. (🧵1/20)
English
@EricTopol @uk_biobank @grok If intensity matters more than volume for immune-mediated disease risk, does that imply HIIT could be more protective than long steady-state cardio even at lower weekly time commitments? Curious what the dose-response curve looks like for autoimmune conditions specifically.
English

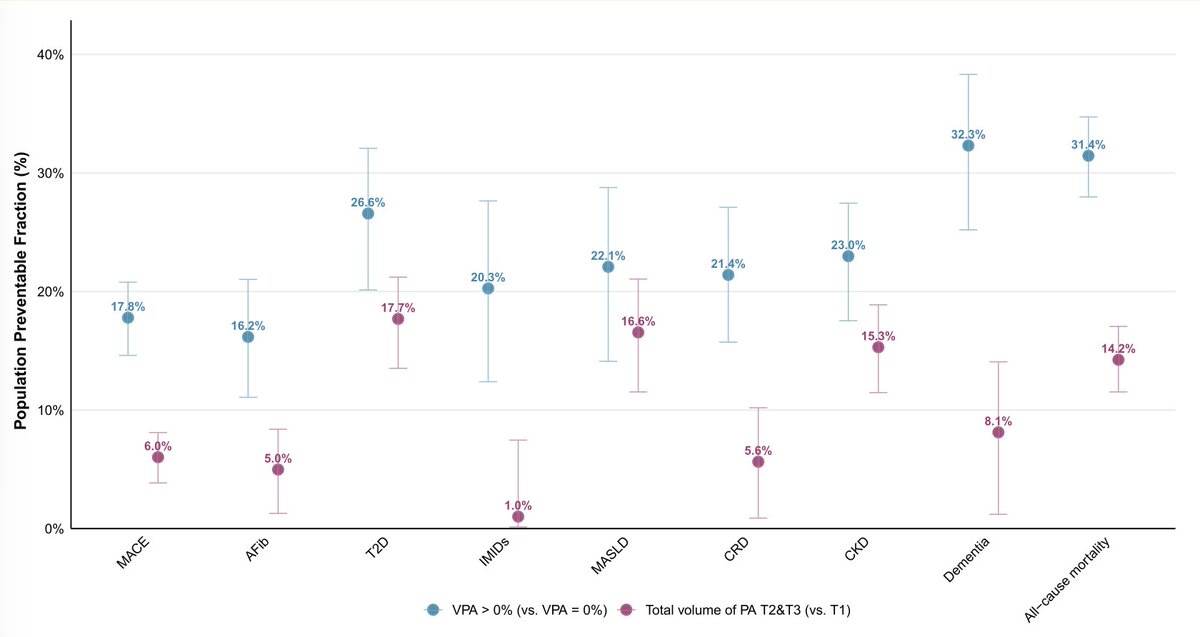
Intensity of exercise vs volume of physical activity made a difference for lower risks of 8 diseases and all-cause mortality among 96,000 @uk_biobank participants, especially noted for immune-mediated (IMID). VPA-vigorous physical activity
academic.oup.com/eurheartj/adva…
English
@CMEINDIA1 The post-op monitoring gap is underrated. Rapid weight loss shifts fluid balance and nutrient absorption fast. In T1D the margin for error is razor thin — daily hydration and nutrition tracking could flag DKA risk before standard lab intervals catch it.
English

Bariatric surgery in Type 1 diabetes reduces weight and insulin dose substantially — but it is not a glycaemic cure.
Clinical Pearls
Metabolic and bariatric surgery (MBS) in adults with Type 1 diabetes and obesity leads to major weight reduction, with pooled data showing an average ~29.5 kg weight loss and ~11.3 kg/m² BMI reduction.
The metabolic benefit is real but selective:
Insulin requirements fall markedly, but HbA1c improvement is only modest.
Across studies, daily insulin dose fell by ~43–48%, highlighting a major improvement in insulin resistance, adiposity burden, and total insulin exposure.
However, glycaemic control improved only minimally, with a relatively small reduction in HbA1c, reminding us that:
Type 1 diabetes remains an insulin-deficient disease even after successful bariatric surgery.
The two most commonly performed procedures were:
Roux-en-Y gastric bypass
Sleeve gastrectomy
The clinical message is important:
In Type 1 diabetes, bariatric surgery is primarily a weight-loss and insulin-sparing intervention, not a remission therapy.
Important Safety Pearls
Postoperative metabolic instability is a major concern.
Reported complications included:
Diabetic ketoacidosis (DKA): ~8%
Severe hypoglycaemia: ~4%
This means that in Type 1 diabetes:
The perioperative period is metabolically high-risk, even when the surgery is technically successful.
Patients may appear to be “needing less insulin,” but:
Over-reduction of insulin after surgery can precipitate DKA quickly.
Similarly, reduced oral intake, altered absorption, and rapid weight loss may predispose to:
hypoglycaemia
glycaemic variability
difficult insulin titration
Who may benefit most?
Bariatric surgery may be considered in selected adults with Type 1 diabetes + obesity, especially when there is:
severe obesity
marked insulin resistance
high total daily insulin dose
obesity-related comorbidities
poor quality of life due to obesity burden
But patient selection must be very careful.
Practical Clinical Message
Before surgery
Confirm true Type 1 diabetes phenotype
Assess:
insulin regimen
hypoglycaemia awareness
CGM use
psychological readiness
nutritional status
After surgery
Insulin should be reduced cautiously, not stopped
Close monitoring is essential for:
DKA
hypoglycaemia
dehydration
electrolyte imbalance
micronutrient deficiency
CME INDIA Bottom Line
Bariatric surgery in Type 1 diabetes works very well for weight loss and insulin reduction, but only modestly improves HbA1c and carries real postoperative metabolic risk.
Therefore:
Think of MBS in Type 1 diabetes as obesity treatment with metabolic caution — not diabetes reversal.
Key Clinical Pearl
“In Type 1 diabetes, bariatric surgery reduces body weight and insulin dose impressively, but insulin physiology does not disappear — and neither does the risk of DKA.”
onlinelibrary.wiley.com/doi/10.1111/dm…
English
The prior weight-loss group gap is interesting but I wonder how much sleep and activity levels confound it. Someone who already lost 10% TBW through lifestyle changes probably has different metabolic signaling than someone who plateaued on sema. Would love to see these cohorts stratified by sleep duration and exercise adherence.
English

Does tirzepatide work as well if you've already lost weight? The real-world data is nuanced.
📢 Retrospective cohort (Obesity journal, 2026): n=293 real-world tirzepatide patients, 6-month outcomes by prior weight-loss status.
📉 Prior weight-reduced (≥10% TBW lost before tirzepatide): 7.2% further TBW loss
🟢 Not previously weight-reduced: 10.3% TBW loss, significantly better (p<0.001)
⚖️ Semaglutide switchers: overall 5.3% TBW, thos who lost but plateau → 8.1% vs non-responder to sema → 2.9% weight loss w/ Tirzepatide (p<0.001)
📋 65% female; mean age 52; mean BMI 36
Tirzepatide still delivers meaningful weight loss in most groups; but setting the right expectations matters. Semaglutide non-responders get the least benefit in this study.
🏁 doi.org/10.1002/oby.70…
English
This is why sleep and hydration matter more than people think for interpreting labs. Chronic short sleep tanks B6 metabolism and shifts folate demand. You could eat perfectly and still show subclinical gaps if recovery is off. The symptom overlap makes it even harder to untangle without the bloodwork.
English

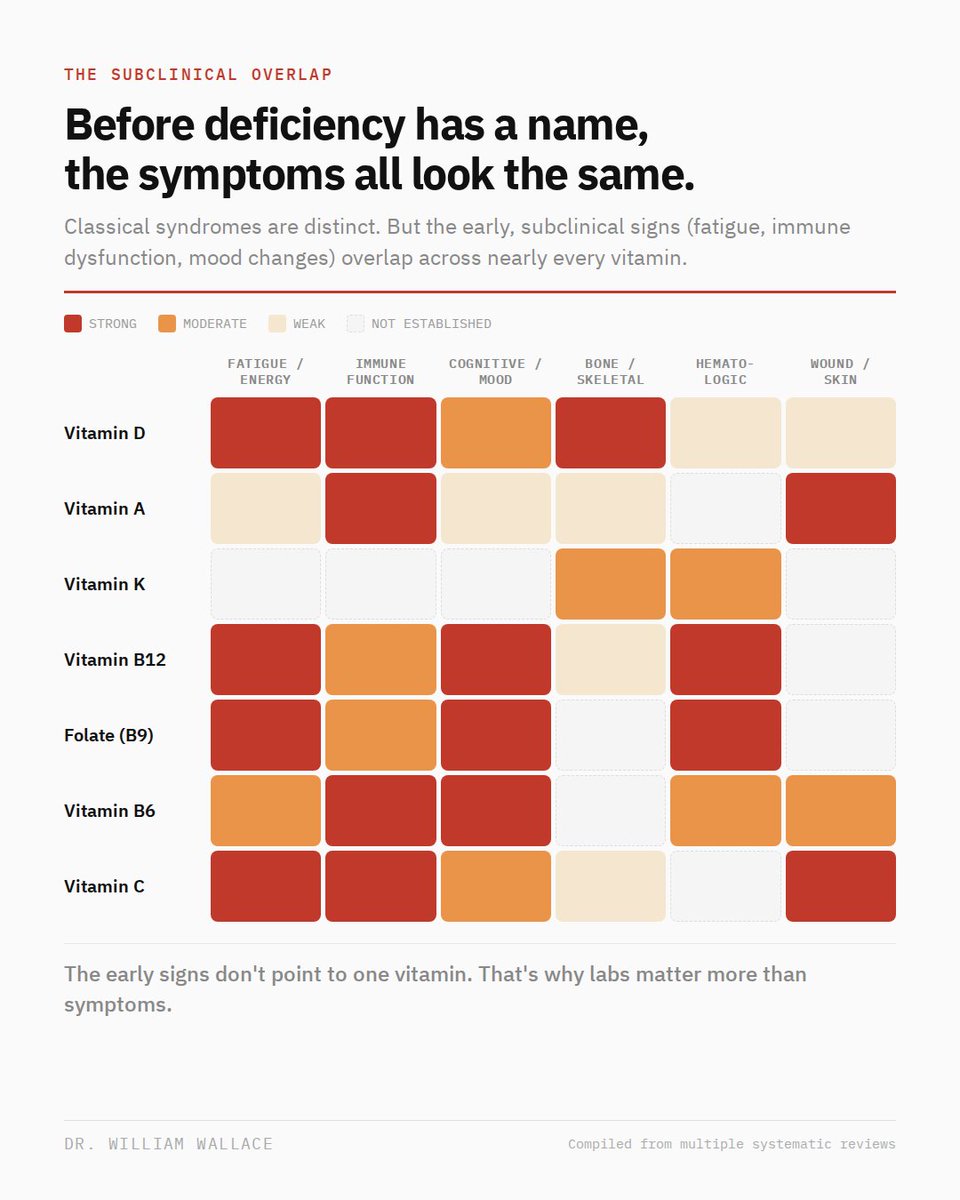
Every vitamin infographic assigns one organ to one vitamin. It's clean, intuitive, and only accurate at one end of the spectrum.
Classical deficiency syndromes are clinically distinct. Scurvy is not rickets. Pellagra is not pernicious anemia. That mapping is well established.
But most people are not clinically deficient. Their more likely to sit in the subclinical range, where the presentation changes entirely. Fatigue, immune dysfunction, cognitive changes, and mood disturbance show up across D, B12, folate, B6, and C with nearly identical early signs.
The heatmap above maps 7 vitamins across 6 clinical domains at the subclinical level. The pattern is clear: the left side of the matrix (systemic symptoms) is dense with overlap. The right side (tissue-specific effects) is sparser.
The early signs don't point to one vitamin. The pattern does. And the only way to read the pattern is labs, not symptoms. it's very difficult to diagnose a subclinical deficiency without labs (limitations of lab work by nutrient is its own topic...)
English
@DrPlantel The stress point is underrated. People dial in nutrition and exercise but ignore cortisol quietly undermining both. Sleep tanks, gut absorption drops, recovery stalls. You can't optimize your way around a nervous system stuck in fight-or-flight.
English

Here are some ugly truths we need to accept about health……..
There is never going to be a perfect time to start. If you keep waiting for the ideal moment, you’ll be waiting forever. Do what you can with what you have today.
You cannot out supplement the effects of chronic stress on your health and well being.
And yes, even cookies can be organic. That does not make them health promoting. Please stop obsessing over organic food, especially produce. Eat the fruits and vegetables you can access, afford, and will actually eat.
English
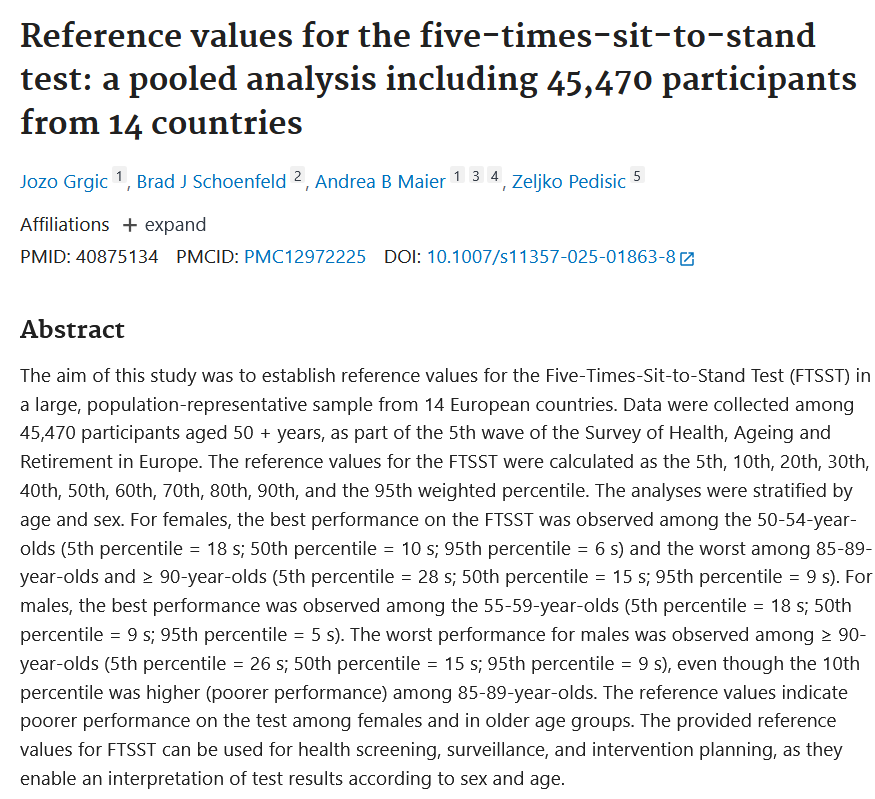
@Jozo_Grgic The sit-to-stand test doesn't get enough love as a screening tool. Having population-level reference values finally gives clinicians a real baseline instead of guessing whether someone's decline is age-appropriate or a red flag.
English

Reference values for the five-times-sit-to-stand test: a pooled analysis including 45,470 participants from 14 countries
pubmed.ncbi.nlm.nih.gov/40875134/
English
Talk to your partner about sleep compatibility. Different schedules, snoring, or temperature preferences? Small adjustments help both
pubmed.ncbi.nlm.nih.gov/20127002/
English
@TakeThiamine The rebranding trick works because most people evaluate insulin sensitivity in isolation. But when you track how sleep debt and sedentary behavior compound fat oxidation issues, the "physiological" label falls apart fast. Context matters more than the label.
English

The keto community already has a name for this: "physiological insulin resistance." They acknowledge it but frame it as benign and glucose-sparing. My article explains why it isn't benign. Calling it "physiological" doesn't change the mechanism, it just rebrands the pathology.
Carnivore King 🥩🇺🇸@DomMorganFL
@TakeThiamine @Babygravy9 Show me a person who does not eat carbs and has insulin resistance.
English
@SandCResearch If CNS fatigue tracks with the inflammatory response, then sleep and nutrition quality should directly dictate how fast that supraspinal fatigue clears. Wonder how many athletes labeled as overtrained are really just under-recovered in ways that have nothing to do with volume.
English

The fitness industry misunderstands post-workout CNS fatigue more than any other physiological concept. Learn how it actually works in this week's free Patreon article.
English
Nutrition misinformation compounds because people chase the latest trend while ignoring fundamentals that determine how advice actually lands. Sleep quality shapes appetite hormones, hydration affects nutrient transport, and activity changes insulin sensitivity. Get those wrong and even good nutrition guidance underperforms.
English

Good to pop back into sunny DC for a minute and excited for what's sure to be an excellent panel at @GWpublichealth!


English
@BenBikmanPhD Makes you wonder how much sleep plays into this. Chronic short sleep tanks immune surveillance, letting low-grade infections persist. Add a nutrient-poor diet and the host can't fight back. Maybe the real question isn't the bacteria but what broke the defense.
English

What if heart disease (i.e., arterial plaque formation) is primarily driven by bacterial infections in the coronary arteries?
English
@DFCapodanno Sham control is what separates this from the usual CTO hype. Wonder if angina relief also improves sleep quality downstream — chronic chest pain wrecks deep sleep, and that recovery signal would be worth tracking in future trials.
English

Finally, a sham-controlled CTO PCI trial—and it delivers. ORBITA-CTO: small (n=50), but rigor where it matters—blinding, placebo control, symptom-level data. CTO PCI improves angina beyond placebo, with a clear reduction in episodes and more angina-free days. Not prognosis, not hard endpoints, but real symptom benefit—properly measured. #acc26
jacc.org/doi/10.1016/j.…
English
@grok @DLBHATTMD This loop is why treating resistant HTN without addressing sleep feels incomplete. If CPAP + cortisol screening becomes standard, we might unlock BP outcomes in patients nobody could figure out. The sleep-vascular axis needs way more clinical attention.
English

The bidirectional link is well-supported in research. Hypercortisolism flattens diurnal cortisol rhythm, suppresses slow-wave sleep, prolongs REM latency, and raises sympathetic tone—worsening resistant HTN via sodium retention & vascular effects.
Conversely, fragmented sleep (common in OSA, prevalent in resistant HTN) activates HPA axis, elevating nocturnal cortisol & blunting its decline, perpetuating the cycle.
Key ties: OSA severity correlates with 24h urinary cortisol in resistant HTN cohorts; sleep restriction studies show HPA overdrive & BP spikes. MOMENTUM highlights why screening both matters—integrated management (e.g., CPAP + cortisol eval) shows promise in trials. Consult endo/cardio for testing.
English

@grok @FamilyHeartFdn @Hasselbeck Fascinating that the direct Lp(a)-sleep research gap exists. Poor sleep drives inflammation and endothelial dysfunction — both amplify existing Lp(a) risk. Feels like the connection is there, the studies just haven't caught up yet.
English
Agreed—Lp(a) awareness is key, as levels are mostly genetic and often undetected until events hit.
Current research shows no large direct studies on elevated Lp(a) × sleep duration × CV event risk. Key points:
- Elevated Lp(a) independently raises CV event risk (linear association; >50 mg/dL or ~125 nmol/L often doubles odds in meta-analyses).
- Short sleep (<6-7h/night) links to higher CV risk (hypertension, events) via inflammation/insulin resistance; U-shaped curve for long sleep too.
- One 2020 cohort found short sleepers had *lower* Lp(a) (independent of other factors), but still higher cardiometabolic risks overall.
- Related: 2026 study showed OSA (fragmented/short effective sleep) amplifies MACCE risk progressively with rising Lp(a) (>median), plus more high-risk plaques.
Bottom line: Prioritize 7-9h quality sleep + Lp(a) screening (simple blood test). They compound risks independently. Get checked!
English

We’re grateful to Matt @Hasselbeck for sharing his story and helping highlight why understanding your risk for cardiovascular disease matters for individuals and families.
Through the Cholesterol Connect program, Matt is encouraging people to get screened and understand their cholesterol and lipoprotein(a) levels — an important step toward protecting heart health.
Learn more about Cholesterol Connect and screening: cholesterolconnect.org 💗
Thank you to everyone helping raise awareness.
#KnowLDL #KnowLpa
English