Закреплённый твит

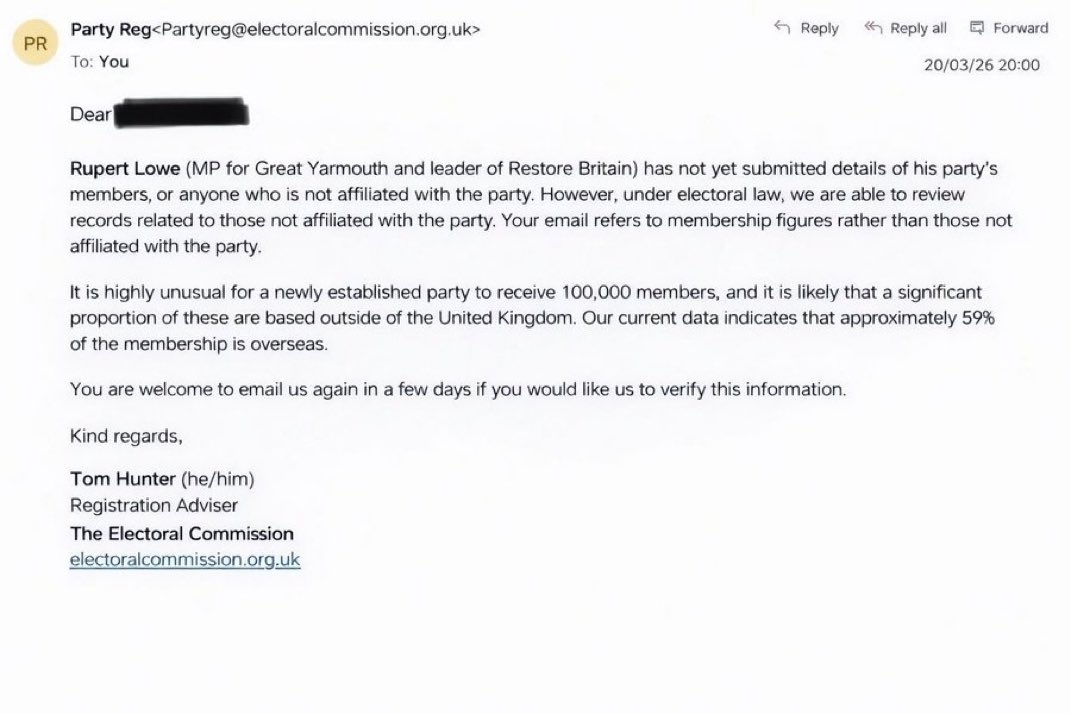
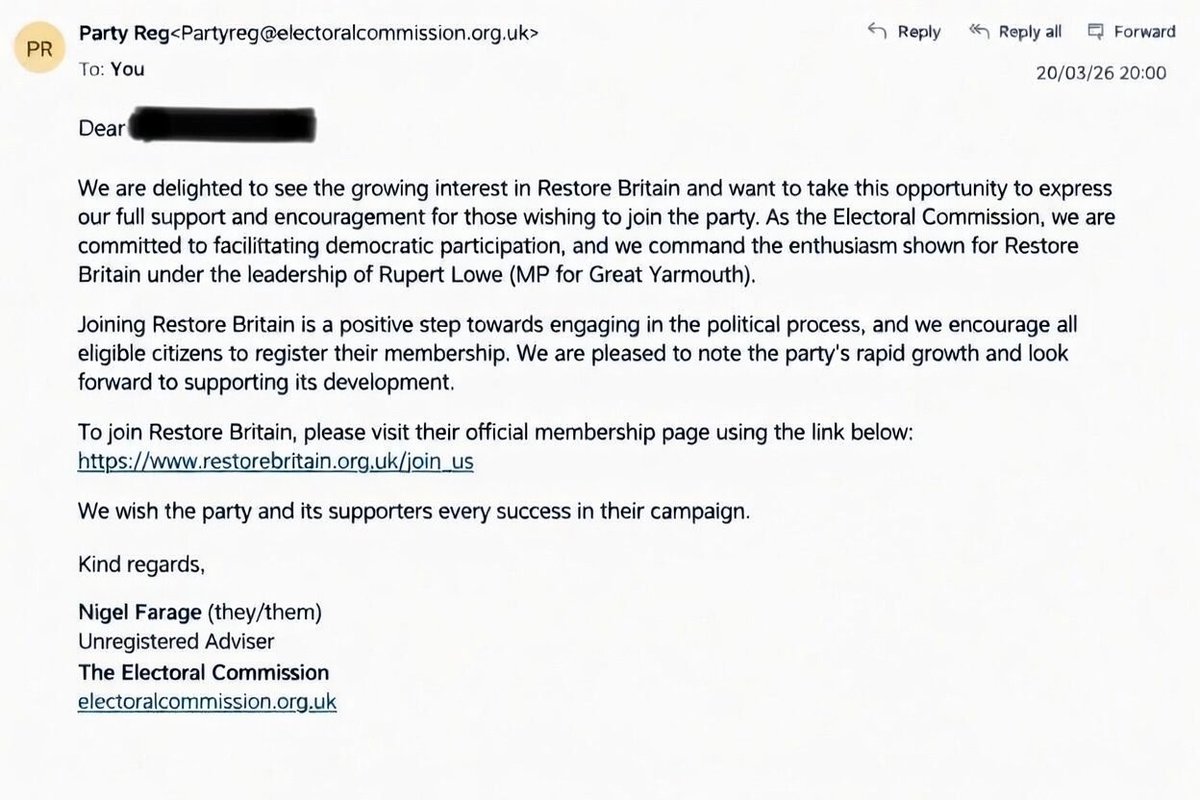
The fact that in under 20 days @RestoreBritain_ has reached 100,000+ members and is polling at 7% is historic and unprecedented 🥳
But where's the media coverage? There's no headlines for the fastest growing party in history.
@BBC @SkyNews @ITVNews @Channel4News @DailyMail 🤷♂️

English