Dr. Vrushali Mahajan Deshpande รีทวีตแล้ว

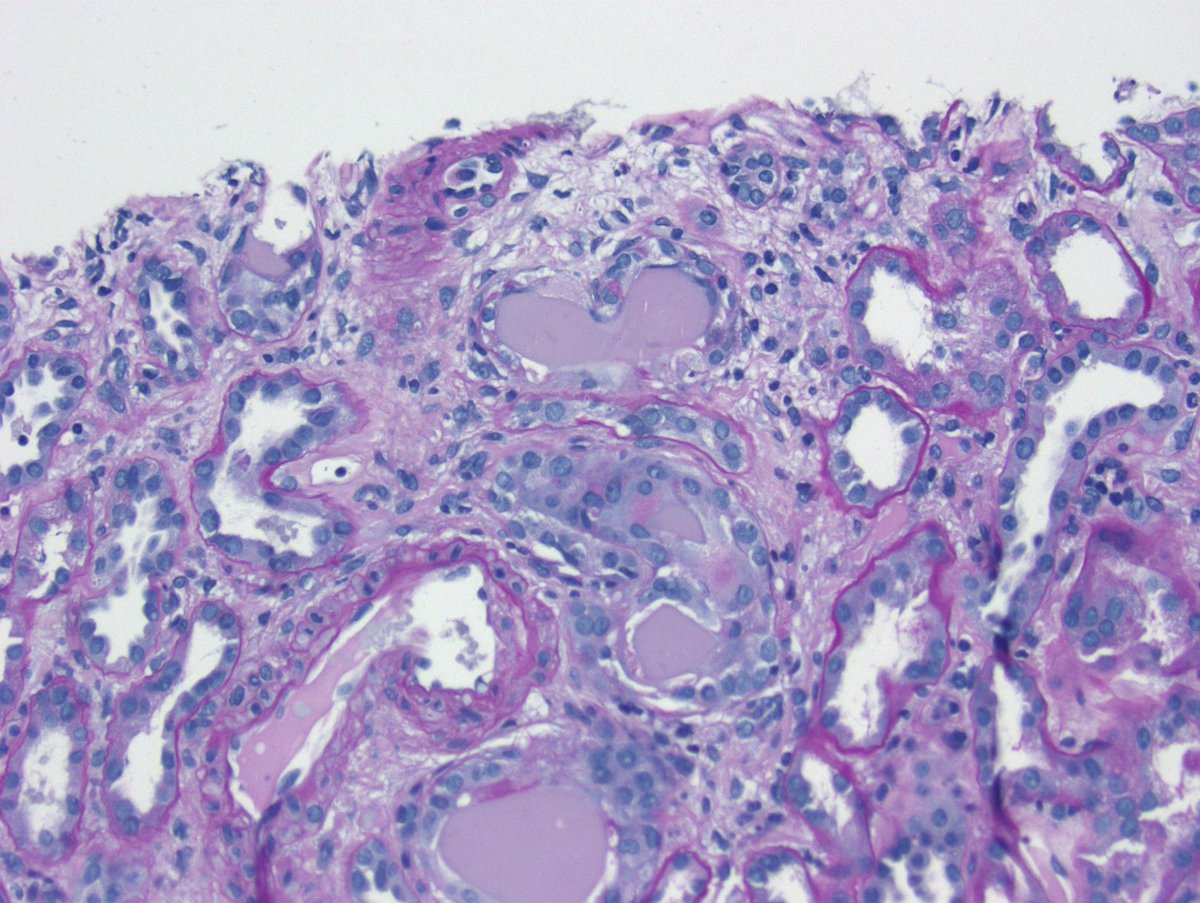
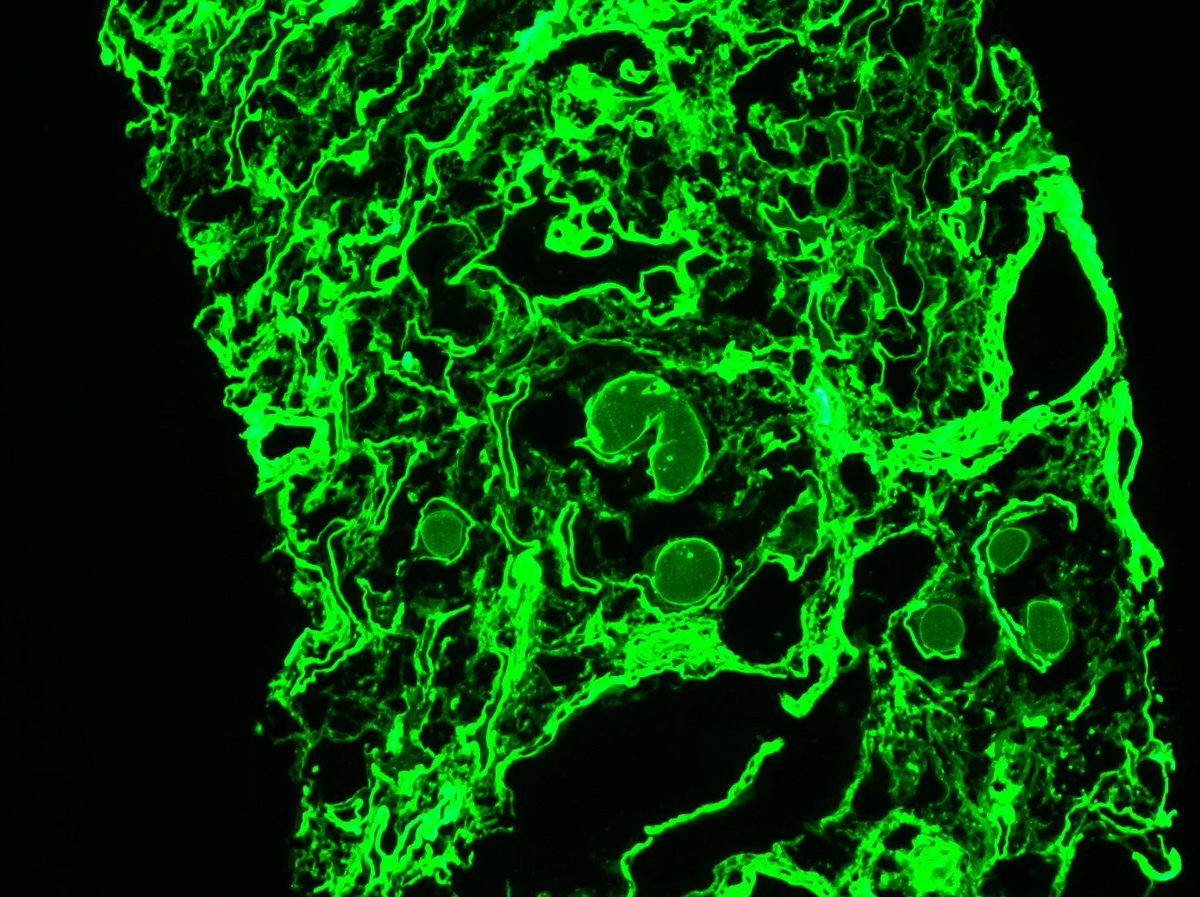
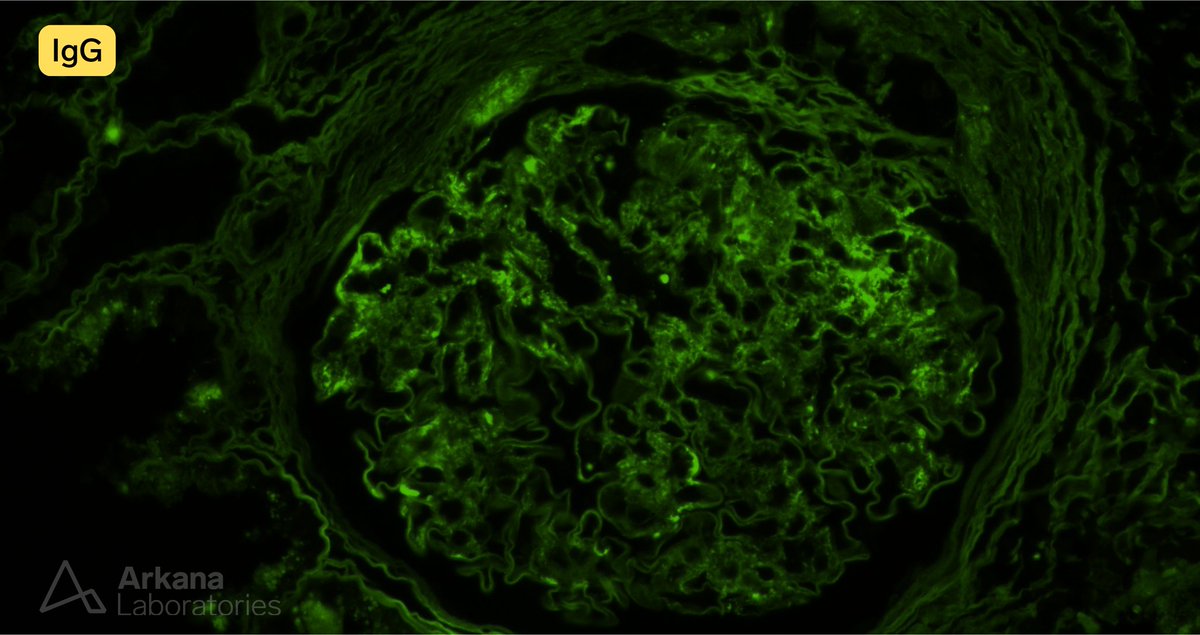
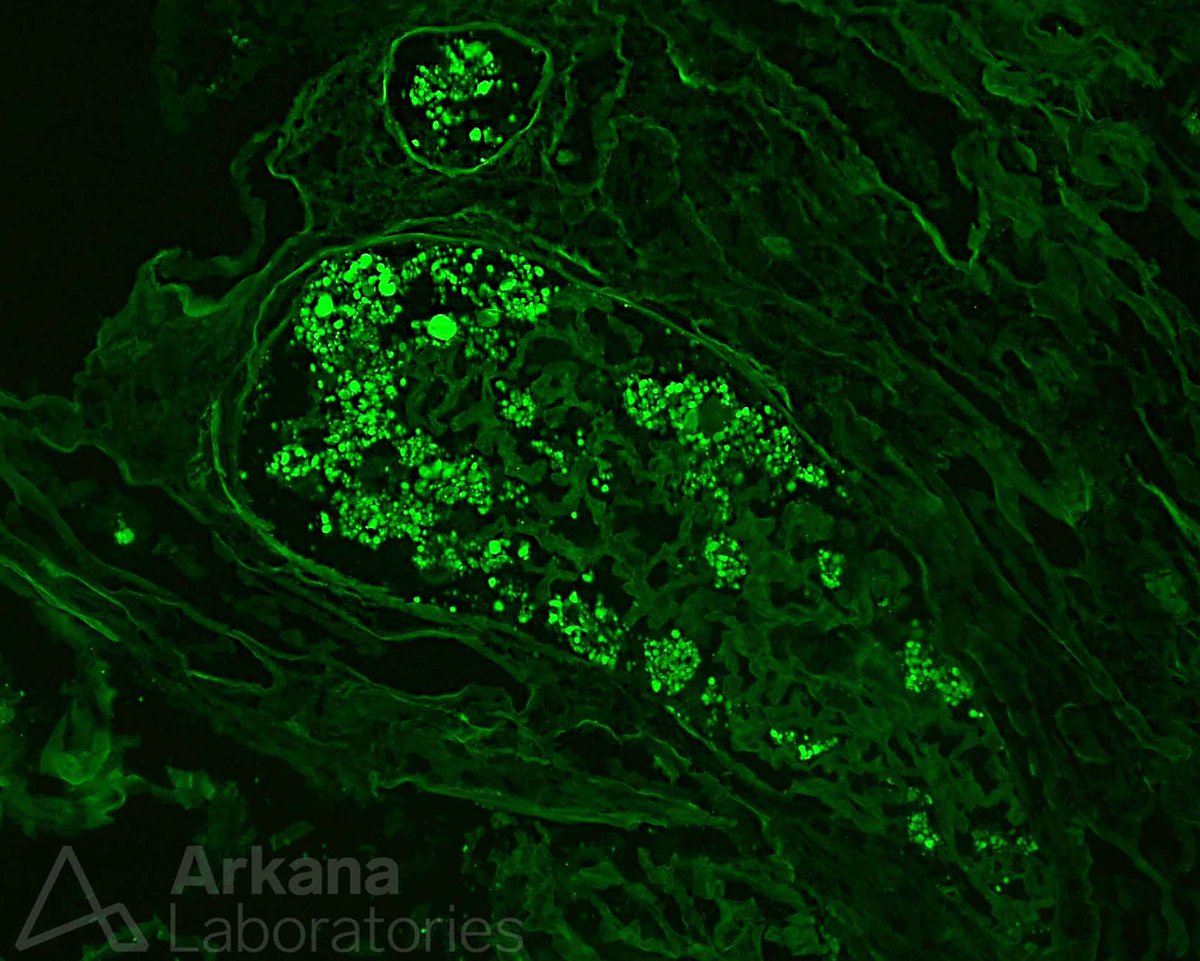
Disappearing glomeruli: loss of linear IgG in anti-GBM nephritis
kidney-international.org/article/S0085-…
English
Dr. Vrushali Mahajan Deshpande
266 posts

@VrushaliPatho
Pathologist by heart. Consultant Renal and Transplant Pathology @Institute of Surgical Pathology, Nagpur. PDCC Renal and Tx Pathology, Advanced ISN ANIO CNC.

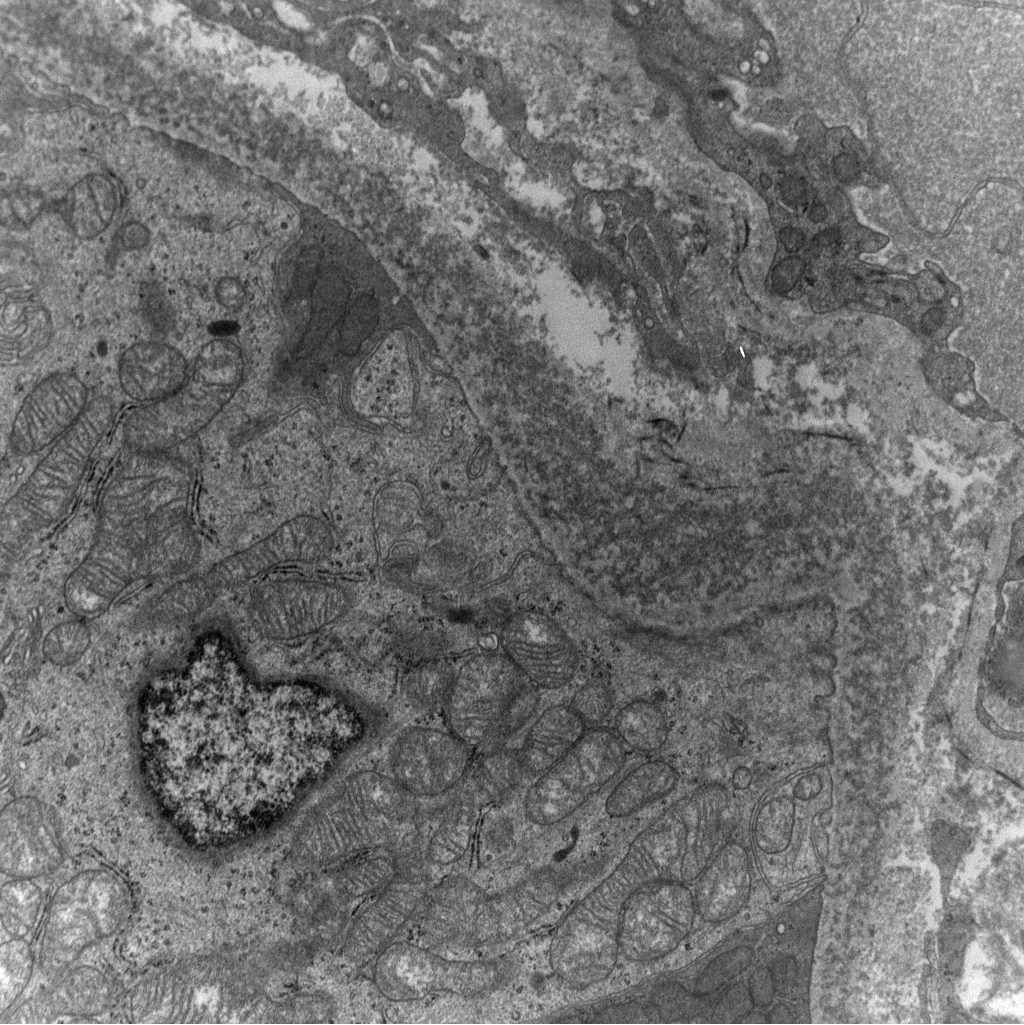
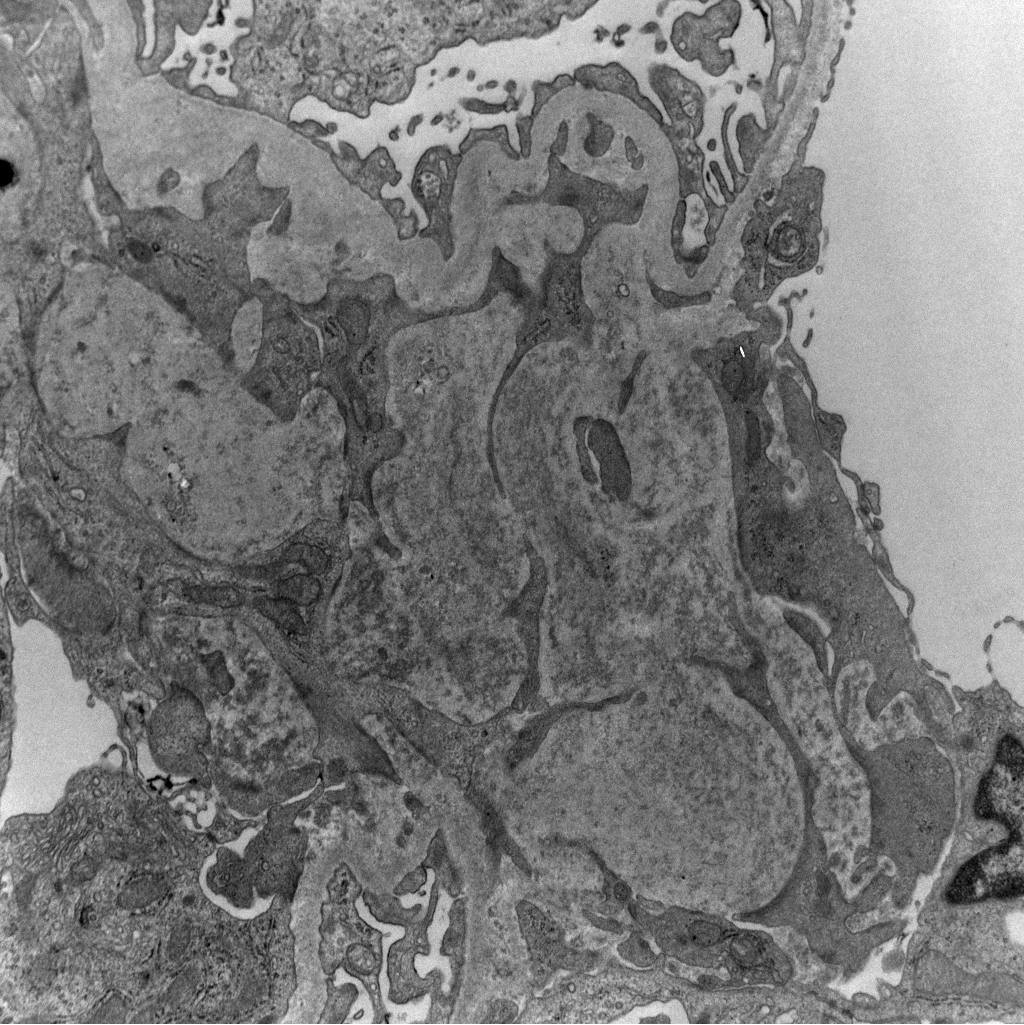
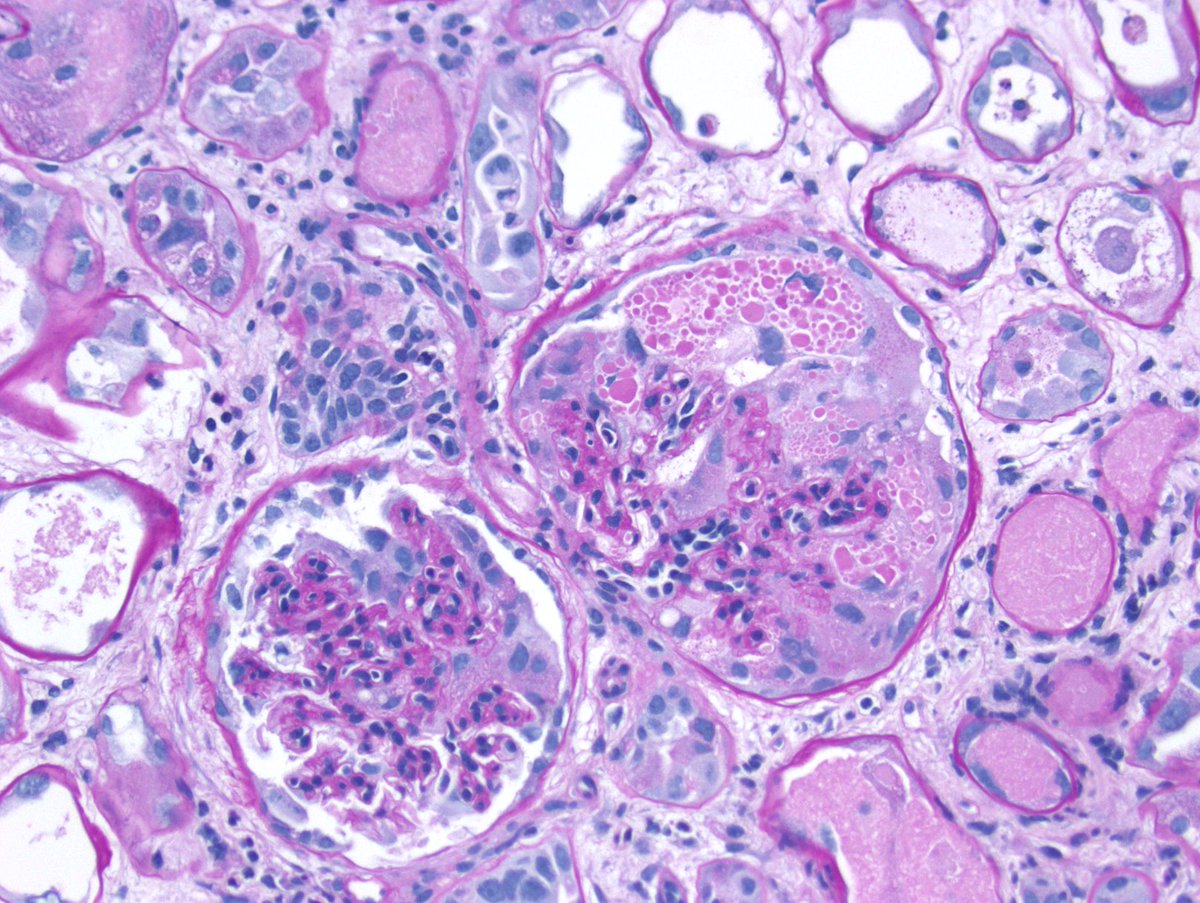
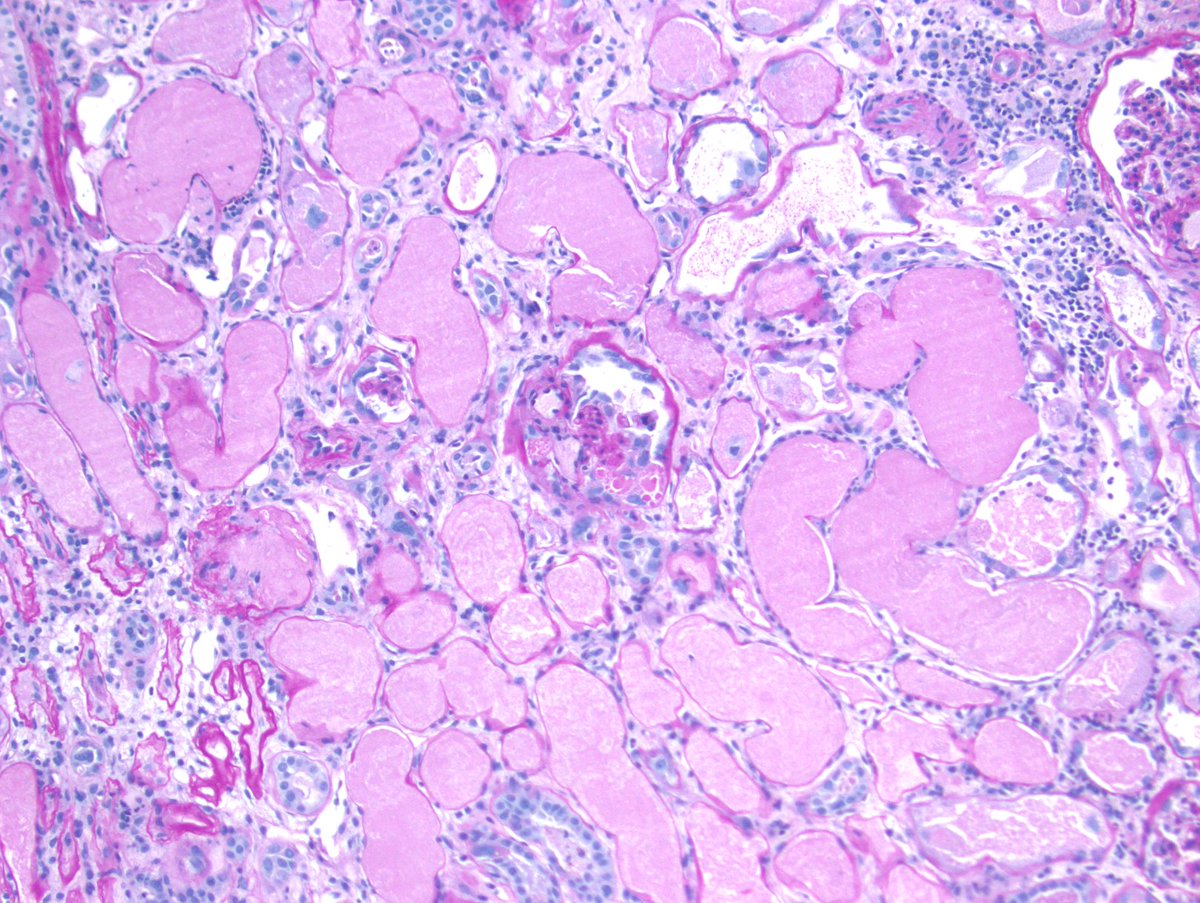
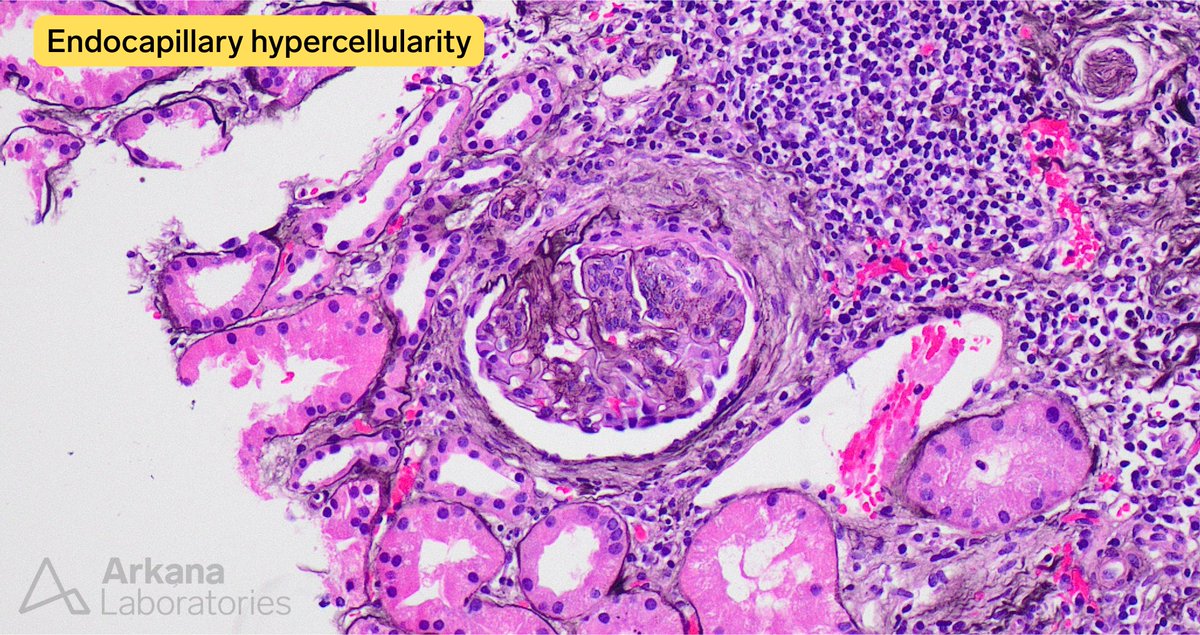
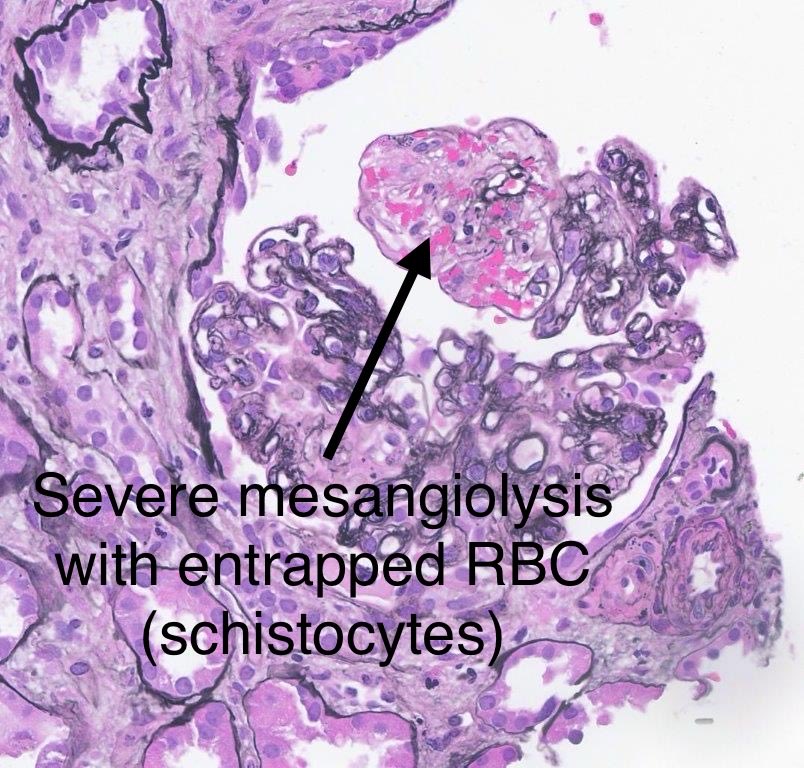
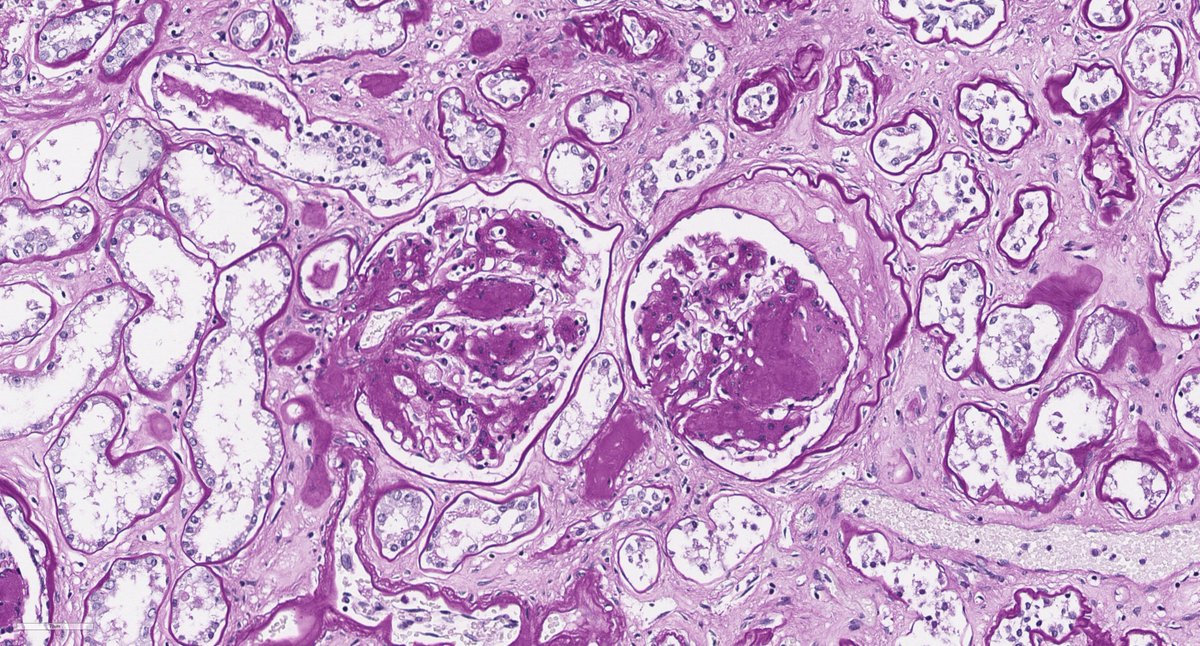
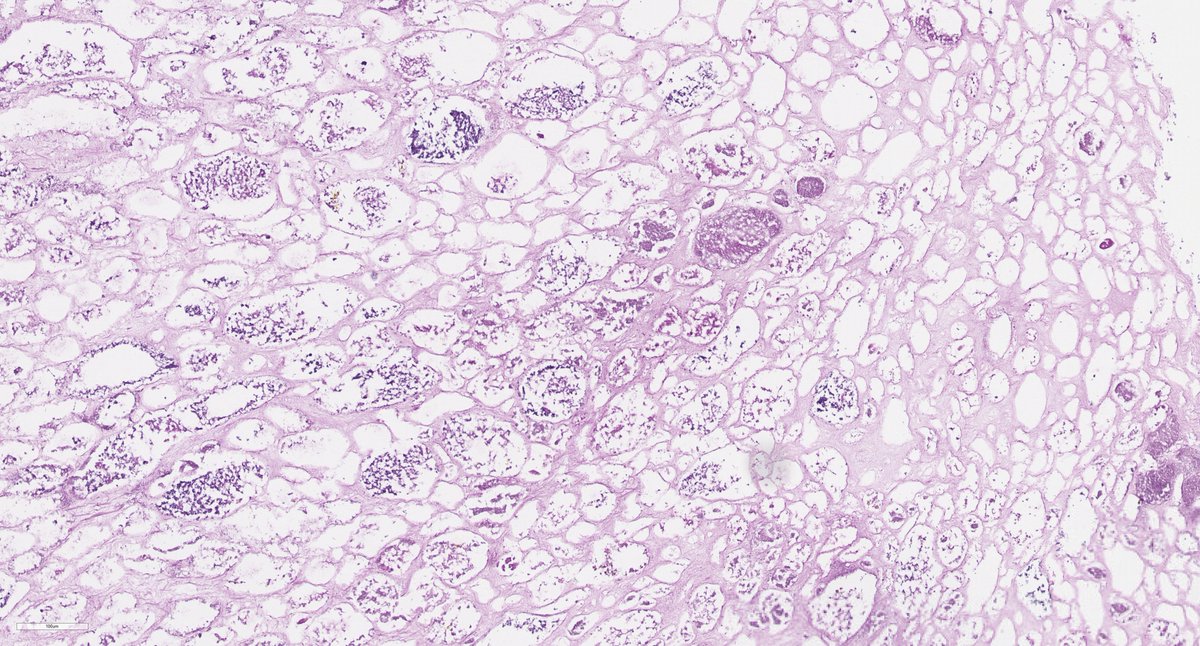
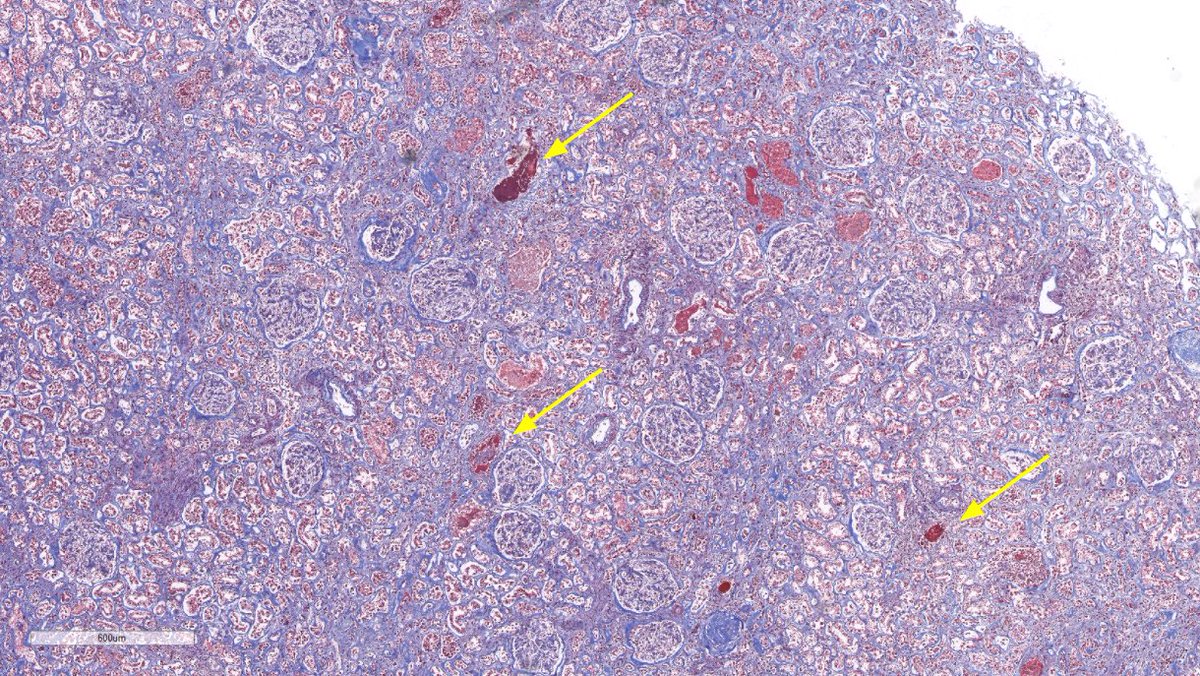
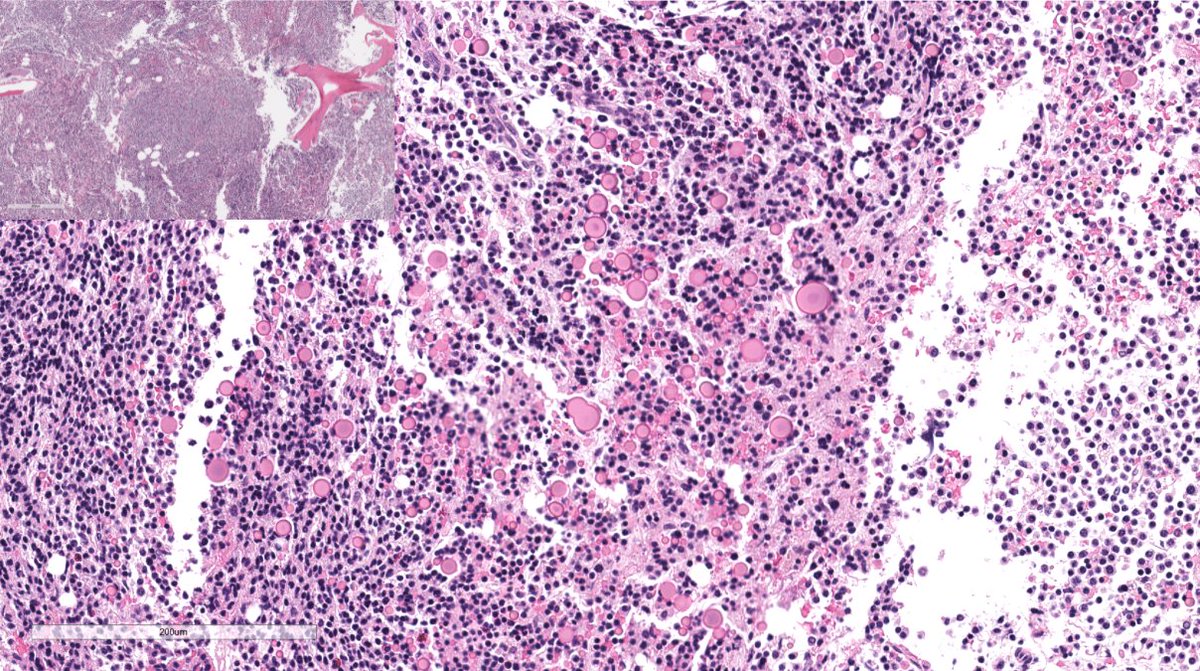
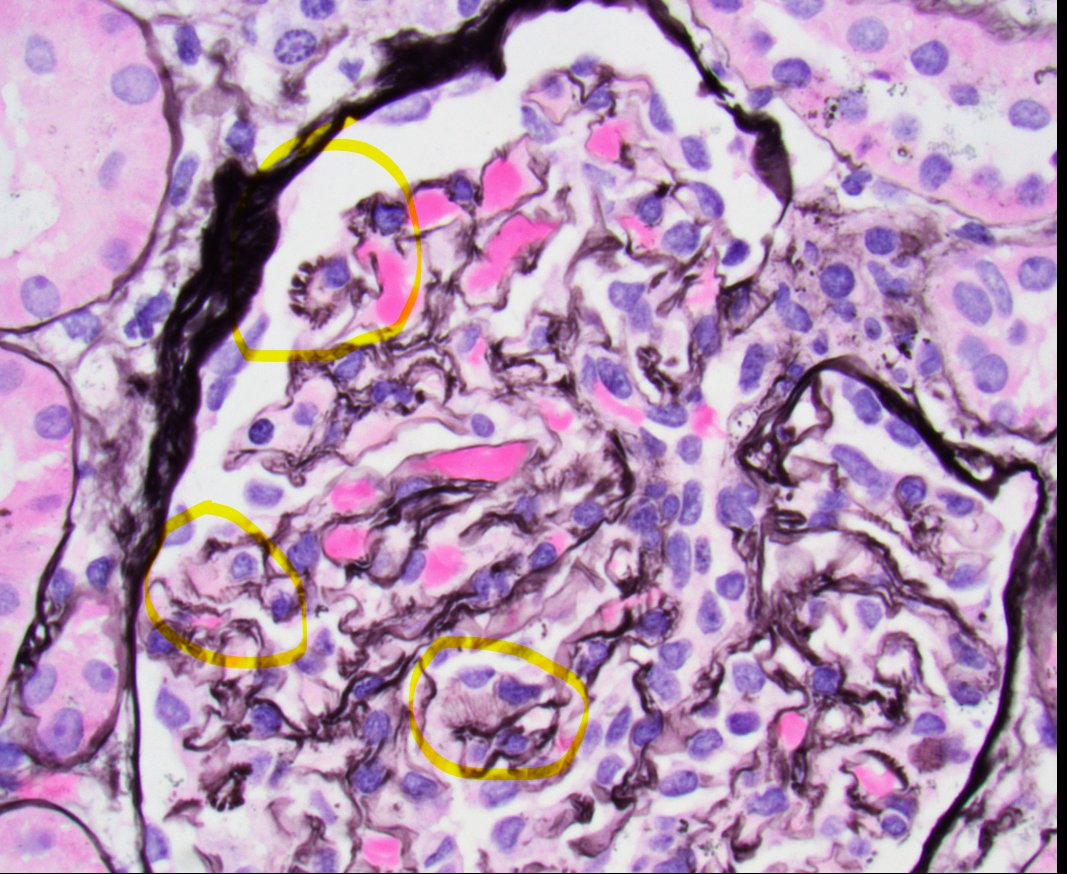
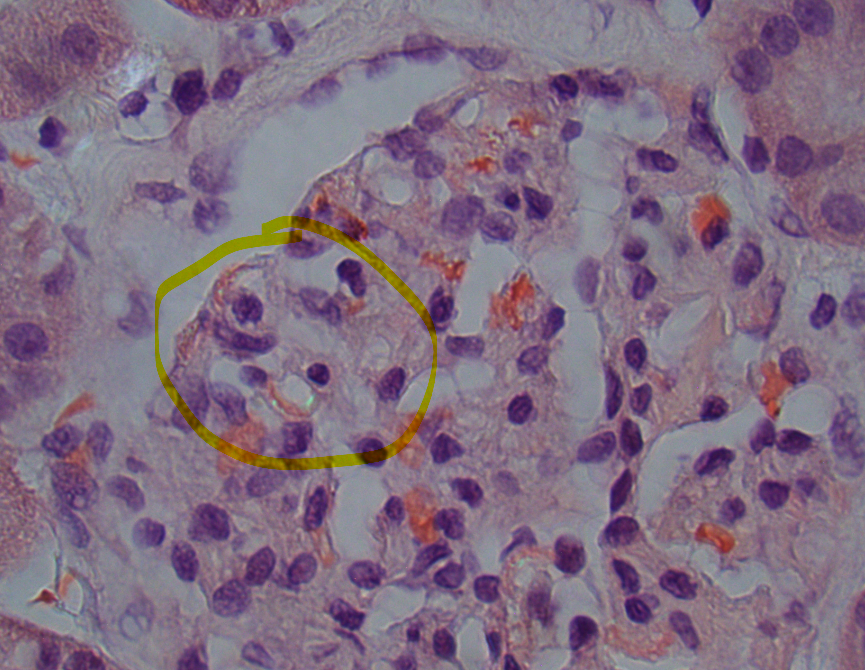
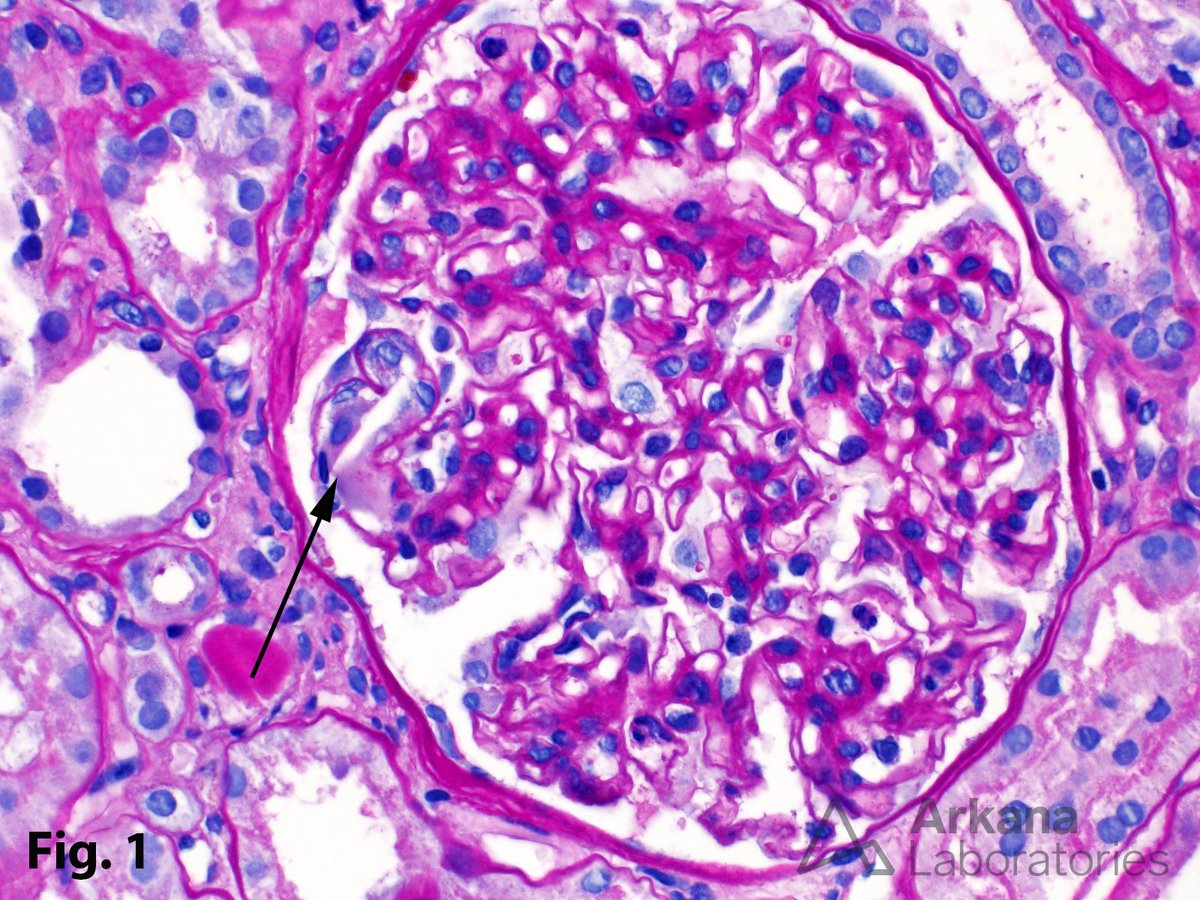
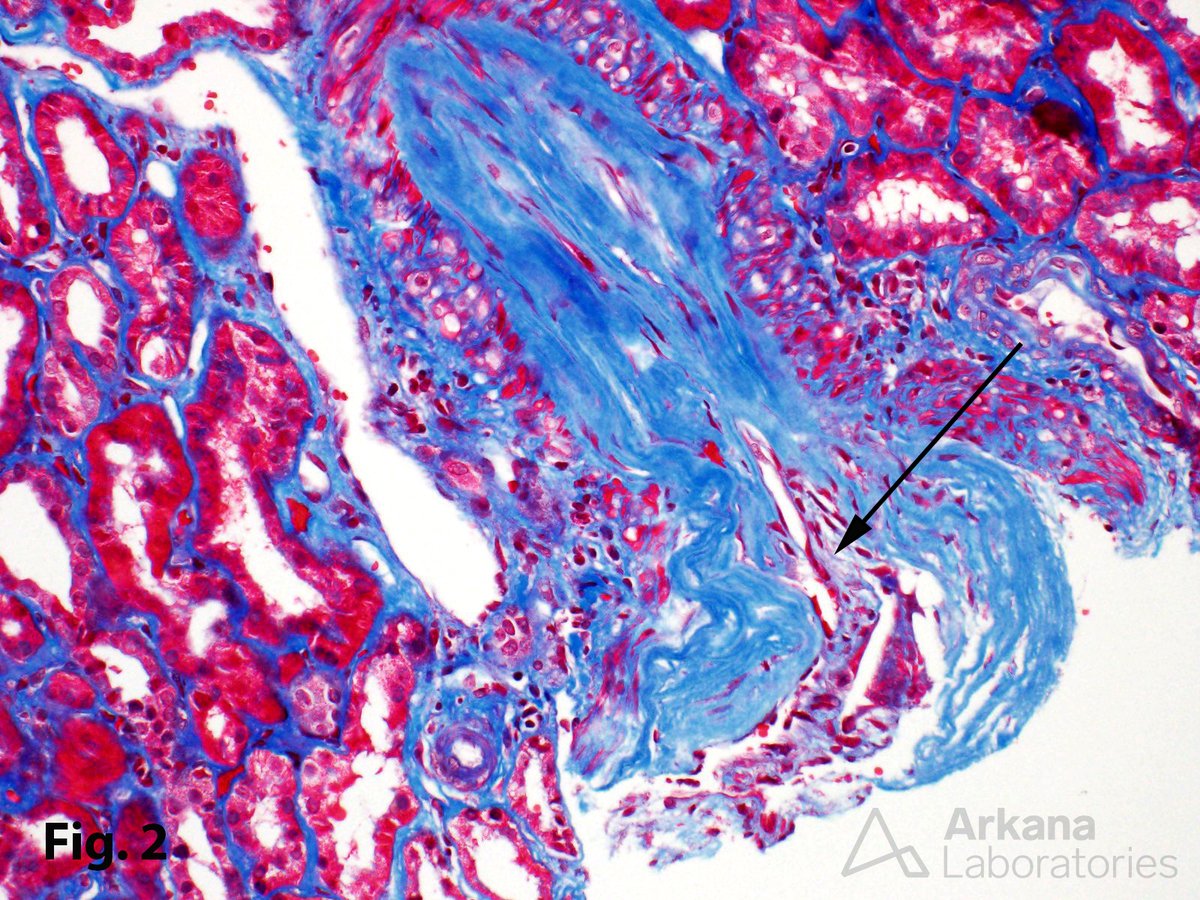
In a patient with subnephrotic proteinuria, negative immunofluorescence, and segmental foot process effacement, what is your diagnosis? #DiagnoseThis #nephtwitter #pathtwitter #renal #kidneypath