ทวีตที่ปักหมุด

Atrial Repolarization
As physicians, we use the electrocardiogram (ECG) almost daily, and electrophysiologists rely on it during surgical procedures. Yet, the ECG continues to hold many mysteries. Today, we will explore the first mystery of the ECG: Where is atrial repolarization? Why is it not visible? It is not addressed in textbooks or electrophysiology literature. Does it exist? If so, why is it not displayed?
As is well known, the P wave of the ECG represents atrial depolarization in each heartbeat. Where there is depolarization, there must be repolarization, yet the ECG does not display it. Some physicians suggest that repolarization occurs in the P-R segment, which appears horizontal. However, repolarization should manifest as a negative wave, given that depolarization (the P wave) is a positive wave. This mystery lies hidden within the heart: the ECG records atrial depolarization as the P wave, but why is repolarization not recorded?
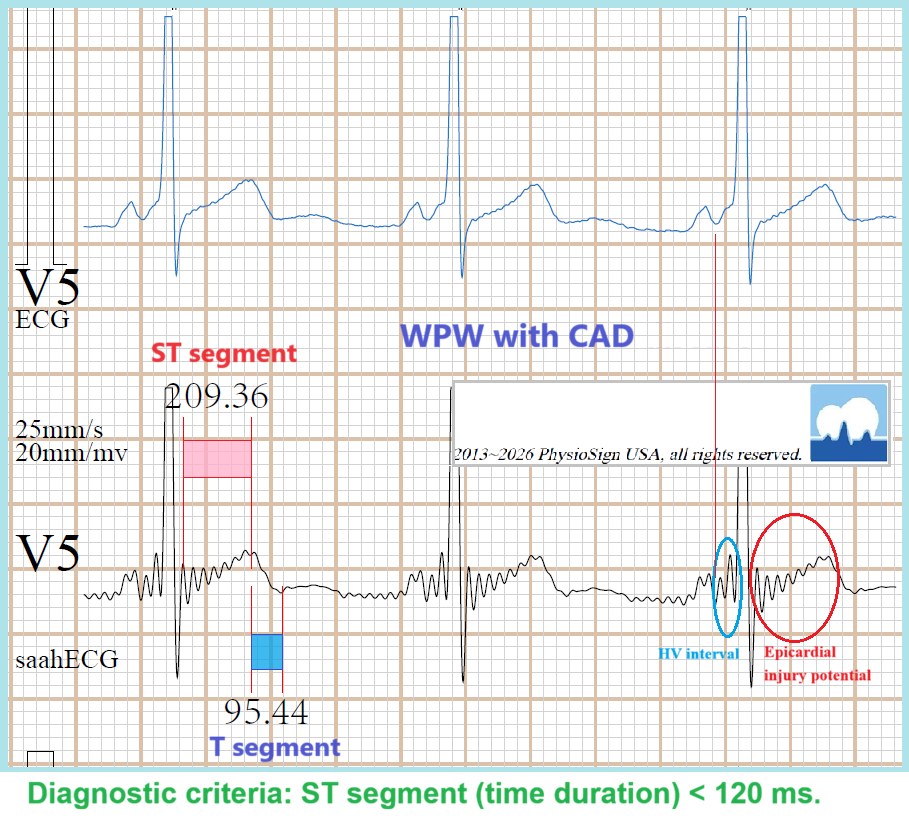
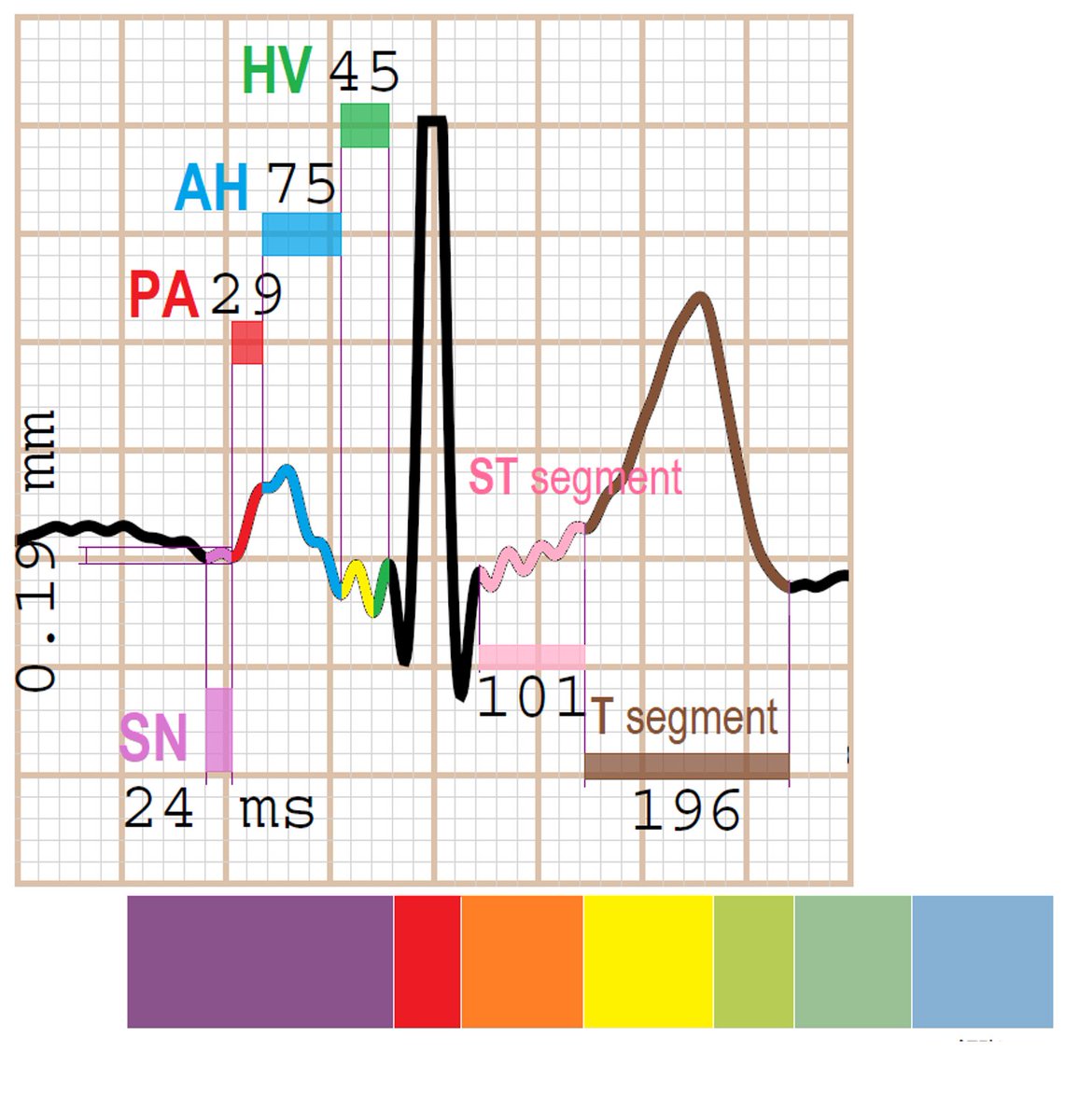
In 2017, electrophysiocardiograms (EpCGs) were recorded for the first time in the PhysioSign Lab. These revealed, for the first time, electrophysiological electro-structure graphs of the entire heart—a map of human life. The essence of life is the vitality of the heart, driven by its electrical activity. The EpCG unveils many of the heart’s mysteries, starting with the location of each heartbeat, which originates definitively from the sinoatrial node (SAN), the source of every heartbeat (to be continued in our next discussion). From the EpCG images, the first secret revealed is atrial repolarization. Consider the image: atrial depolarization and repolarization are both recorded, whereas the conventional ECG only shows atrial depolarization.
The EpCG uncovers the secrets of the ECG. As a continuous recording system, it provides a deep understanding of electrophysiology, analyzing many cardiac mysteries for the first time. Unlike invasive techniques, which capture only local point potentials, the EpCG reveals the full scope of the heart’s electrical conduction. From the EpCG, we observe that the P wave of the traditional ECG compresses the highest atrial frequency—essentially folding all frequency signals into a simplified, string-like representation—while the atrial repolarization signal, the core of the X-axis, remains hidden at the center.
The primary challenge of the ECG is its limited signal display. Unlike medical imaging techniques such as CT, X-ray, or MRI, which provide detailed visuals, the ECG relies on estimation and interpretation. It reveals far less than electrophysiological science demands. Even invasive methods fail to capture the anatomical context, positioning the ECG as one of the oldest and most empirical tools in medical science.
PhysioSign USA
#ekg #ecg #electrophysiology #medtech #innovation #ai #cardiology

English