@DrDiGiorgio @chriswithans Our hospital offers us 42 an hour to take additional call and they wonder why we “pass”…
English
General Buck Turgidson
1.9K posts

@GeneralBuckTur2
“I’m not saying we wouldn’t get our hair mussed, but I am saying 10-20 million people killed tops - depending on the breaks”

Kaiser LA wants to pay board-certified cardiologists $218.65/hr to work overnights and weekends. Don’t take this job. It’s hurts all of us.
@DA_Stockman And what’s in the job description of the Iranian government functionaries who hang gay people for being gay, shoot tens of thousands of peaceful protesters down in the streets, or beat women with billy clubs because they don’t wear a certain style of headscarf?

To everyone who thinks that AI will eliminate the middlemen in healthcare: Remember electronic health records. Everyone assumed moving from paper charts to computers would improve efficiency. Regulations and bureaucracy ensured we got the opposite. It can happen with AI too.

It is psychologically impossible for some doctors to come to the internal recognition that COVID-19 mRNA injections have been a disastrous mistake for their own health, and for the health of their family and their patients.

JUST IN: CEO of NYC Health, America's largest hospital system, says AI could replace “a great deal” of radiologists right now.

@DutchRojas Why don’t you tell me the average margin of an average hospital? Yea they’re just raking it in right? 🤣
Single-payer healthcare. Free childcare. Zero tuition at UCs and CSUs. This is the California we can build when we prioritize working families over corporate profits. I’m standing with UAW 4811 today because you can't have our world-class education system without supporting the people who provide it.



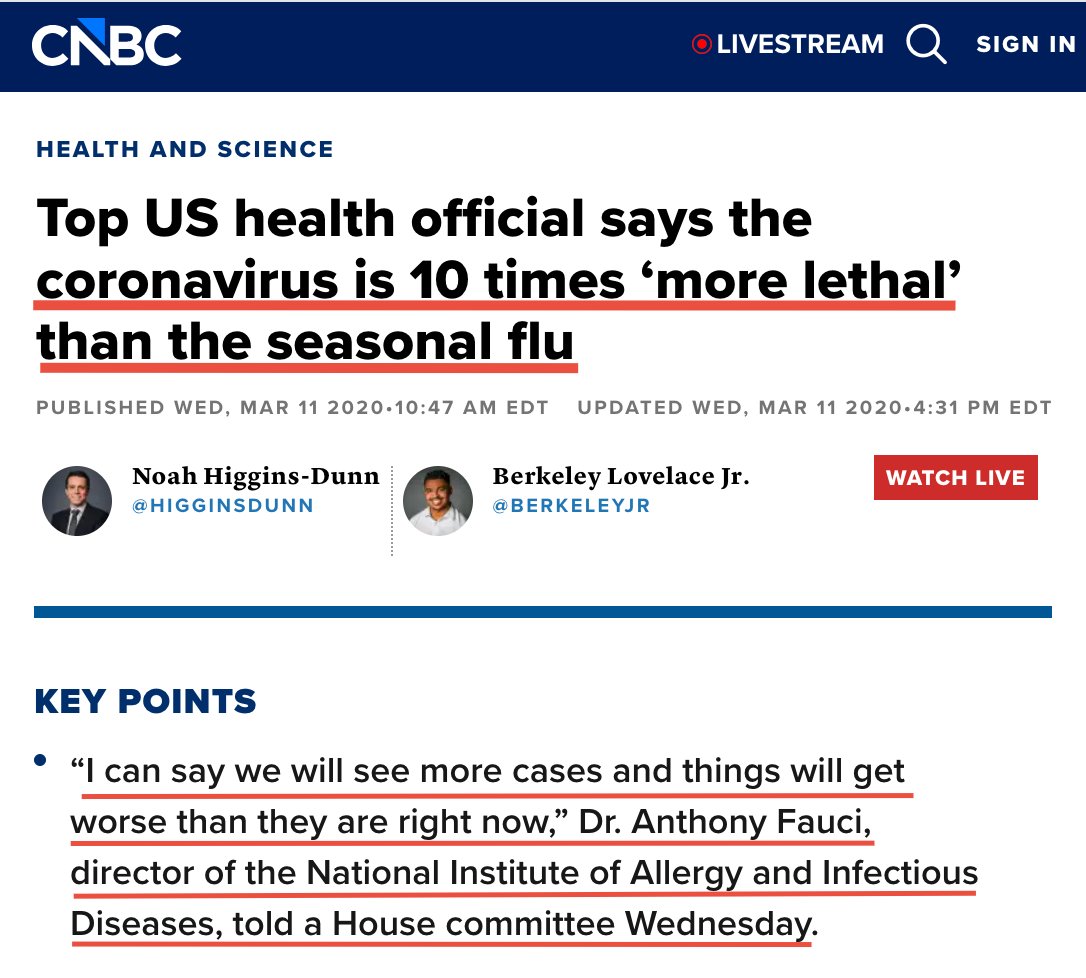

I hate to say it, but I no longer trust doctors. Especially after what they did to millions of people during Covid. Today's doctors seem like they're more concerned with everything else, but our health. Do you trust doctors?


Meanwhile in the real world Heart attack rates and deaths trends since statins widely used
By Feb 2020 we already knew hydroxychloroquine worked. Why? SARS-CoV-2 is ~78% identical to SARS-1, and HCQ had already shown effectiveness against SARS-1. The real question isn’t why doctors used it. The real question is why authorities tried so hard to stop them.


Never leave your loved one alone in the hospital. Every hour you are allowed to be there, if you are able to, I highly recommend being there. Be perfectly cordial with staff. But watch over everything like a hawk. Trust me on this.

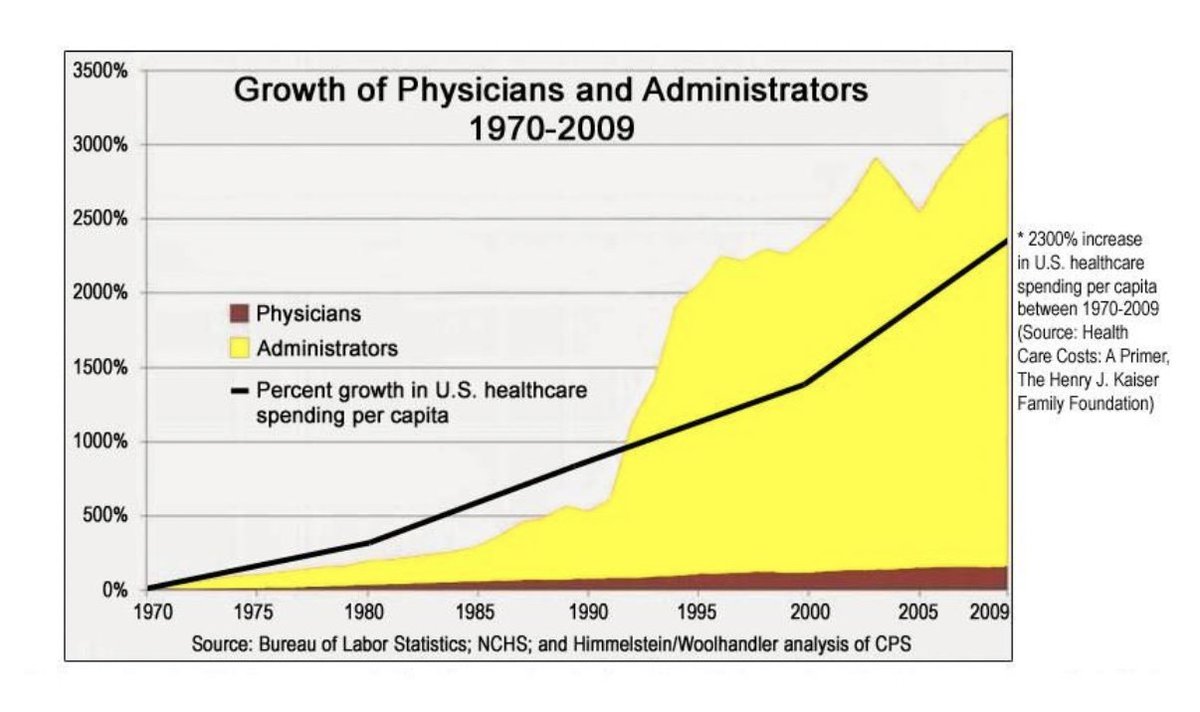
Schools don't have a funding problem, they have an administrator surplus problem