
christopher parks
3.1K posts

christopher parks
@caparks
Husband, Dad to 2 boys. Has a mildly dry sense of humor. Founder/former CEO + CDO of Change Healthcare and 2 other exits. Trying to help others
franklin, tn شامل ہوئے Nisan 2007
224 فالونگ1K فالوورز

Claude Opus 4.6 can contact every decision maker in your market
In just 45 days.
While everyone's obsessed with "AI SDRs" spamming inboxes, we built something different.
Claude as a research copilot. Inside a human-led outbound engine.
We're not automating conversations. We're automating the grunt work that kills productivity.
Here's what it does:
→ Ingests your ICP and past wins
→ Scans raw lead data to surface actual decision-makers (not interns)
→ Pulls 3-5 real signals per account for messaging
→ Outlines multi-contact plays for Tier 1 accounts
Humans still decide who to contact, what to send, and who gets booked.
Claude Opus just handles the spreadsheet hell.
Result: Fewer junk meetings. More calls with people who can actually sign.
I just put together a breakdown covering:
• How we use Claude to clean and filter lead lists
• Our exact prompt structures for decision-maker discovery
• How we combine Claude Opus 4.6 + ChatGPT/Gemini without building a bloated AI stack
• Real workflow examples from our outbound engine
This is the same system we use internally to book qualified pipeline.
No fluff. Just the actual prompts and process.
Want the "Claude Outbound Copilot" breakdown?
1. Connect with me
2. Comment "CLAUDE"
(must be following - RT for priority access)
English
So it's true. I am coming out of retirement. Many of my friends who are on the Payor side of the fence will not be happy with me.
linkedin.com/pulse/im-comin…
English
English

English
To all of my health tech and Provider friends, settle this argument: is it Payors or Payers?
The AMA has officially leaned into Payors and yet, often times, I’ve seen Payers used when speaking about any of the BUCA gang. I prefer Payor but am I right or wrong?
English
@LukasiakLu46027 @grok Waitaminute…. Lucas, did you just “let me google that for you?”
I’m teasing, of course. I, too, did the query via Grok, Claude, and ChatGPT and it appears both forms are acceptable
English

English
My fourth day into a new adventure and appreciative to Teamworthy Ventures for allowing me to join today’s event. Great initial fireside chat w @dtompaine
Yes, I’m coming out of retirement.

English
@StuartBlitz Hahahahahahahaha… wait a minute, that’s happened to me, too. Sigh. Nevermind.
English
There's nothing more annoying when you put off digging into a Google Doc - and then when you finally do? You don't have access.
English

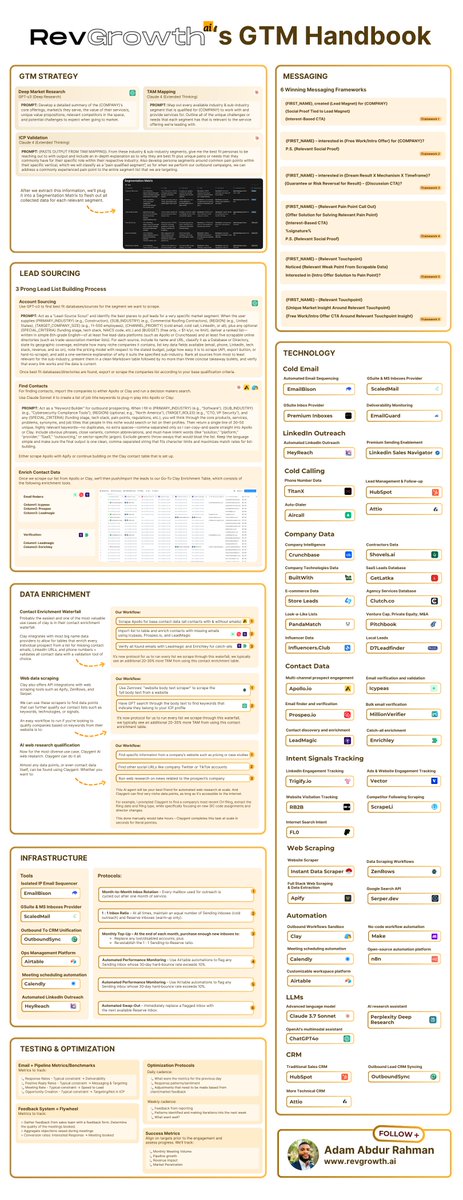
We used this GTM playbook to generate $15M+ in B2B pipeline for our customers in 2025
And threw it all into a PDF for you to steal.
This handbook covers everything from:
> GTM strategy development
> Lead sourcing
> Data enrichment
> Infrastructure
> Testing & optimization
> Messaging
> Technology
Like + Comment "GTM" & I'll DM you the PDF.
English
@StuartBlitz And I’m thinking of something different than just another SaaS portal … crap Stuart, why’d you make me start thinking about this?
English
If someone dropped $50M into your bank account today to build a good health tech business (meaning actual material revenue and margin) - what would you actually build?
Money is no longer a blocker.
English
@StuartBlitz As data is increasingly abundant, Providers are perpetually bad at using, leveraging, and optimizing across their service-line contracting.
English
@StuartBlitz Just a guess…Smaller than large, multi-state IDNs (though could be used to augment existing staff) but bigger than a 4 Dr group
English
@anothercohen Woefully late on acknowledging the sheer brilliance of this flawlessly executed announcement video. It’s so inside baseball that I think it may have made many folks on Sand Hill Road implode.
GIF
English

Excited to share that we've raised a $22.5m Series A for Hello Patient, led by Scale Venture Partners.
This is by far the worst announcement video I've ever made.
I can't believe our lead investor agreed to this
Alex Cohen@anothercohen
Our lead investor and I have a big announcement to share. Thursday, 9AM PT.
English
Much to my disappointment— Philly is just as hot today as it was in Nashville this morning
#WhatWasIThinking
GIF
English
@healthapiguy A well framed and salient post, Brendan. Often, folks get so focused on trying to engineer perfect guardrails for the future that they gloss past that the current problem only needed to be solved for today’s circumstances
English

A uniform truth that will play true: in three to five years, we will look back at the infrastructure we're building today and say "how stupid were we". HL7v2, CDA, FHIR...whatever we think is "the" solution will be superseded. And we'll certainly do that about FHIR.
Each transition typically happens not because the old standard fails at what it was designed for, but because the underlying assumptions about how systems should interact become obsolete. HL7v2 was built for intra-operability within an enterprise. HL7v3 and CDA was built for exchange between care organizations. FHIR was built for modern app development.
FHIR assumes humans (or human-programmed systems) are the primary consumers of healthcare data. So we structure everything around human-readable resources, predefined use cases, and explicit semantic mappings. We spend enormous effort on standardized terminologies, coded values, and structured fields because humans need that scaffolding to interpret and act on the data.
It feels like we're almost at that moment and tipping point. The momentum with FHIR will continue and its utility will remain, but so many of the rigid, use case specific pipes we've built will feel silly as we graduate to the next era of exchange - perhaps MCP, perhaps something we haven't thought of yet, but almost certainly a data exchange mechanism that's LLM/AI native. Dumb, flexible pipes become infinitely more valuable than smart, rigid ones.
To believe otherwise is to believe we've reached an end state that is not just the local maximum, but the absolute zenith of what's possible. The only truth is that the things we've built will look dumb to the next generation.
English
@StuartBlitz Having lived this… I did a spit-take while drinking my coffee and reading this post. Damn you, Stuart ;)
English
Health tech-enabled services founder: We used a bunch of off-the-shelf, 3rd party software since it was just easier
Their infrastructure:

English
@SooahCho @SignalFire So very appreciated, Sooah! Btw… the correct CH twitter account is/was @Change_HC if you want to update the X post.
English

📊 300+ Health & PharmaTech unicorn founders. $1B+ outcomes. One big question: who’s actually building the future of healthcare?
We used @SignalFire's proprietary AI platform, Beacon, to analyze the backgrounds, career paths, patterns across 300+ Health & PharmaTech unicorn founders, and exit paths. 🦄
Here’s what we found:
🌱 58% of them are first-time founders
🔄 45% came from outside the healthcare industry
🤝 80% of them built with co-founders—not solo
📍 25% of them are in the Bay Area, 16% in New York and only 4.5% of them are in Boston
💪 70% had 10+ years of experience
🚀 The most disruptive teams? Lean, AI-native, “Centaur hybrid AI + human teams” blending GenAI talent with seasoned operators
Read the @FierceHealth special report from @HeatherLandi and our report in comments below👇
Becoming a unicorn is rare. Becoming a decacorn is rarer still—fewer than 4% of unicorns hit a $10 billion decacorn valuation.
The elite founders who have crossed that line include:
Peter Gassner and Matt Wallach of @veevasystems Systems
@caparks and Robert Hendrick of @ChangeHealthCa2
Ed Park and Todd Park of @DevotedHealth
John Burd, Scott Glenn, Lauren Otsuki, Ellen Preston, and Bret Megargel (deceased) of @dexcom
Jeff Tangney, @NG, and Shari Buck of @doximity
Dennis Gilling of @IQVIA_global
@GlenTullman of @Livongo
Shoutout to @halletecco, MPH, MBA for her unicorn list, which is featured in the report!🙏
#HealthTech #PharmaTech #AI #VentureCapital #Founders #Unicorn #Decacorn #BeaconData #SignalFire

English