پن کیا گیا ٹویٹ

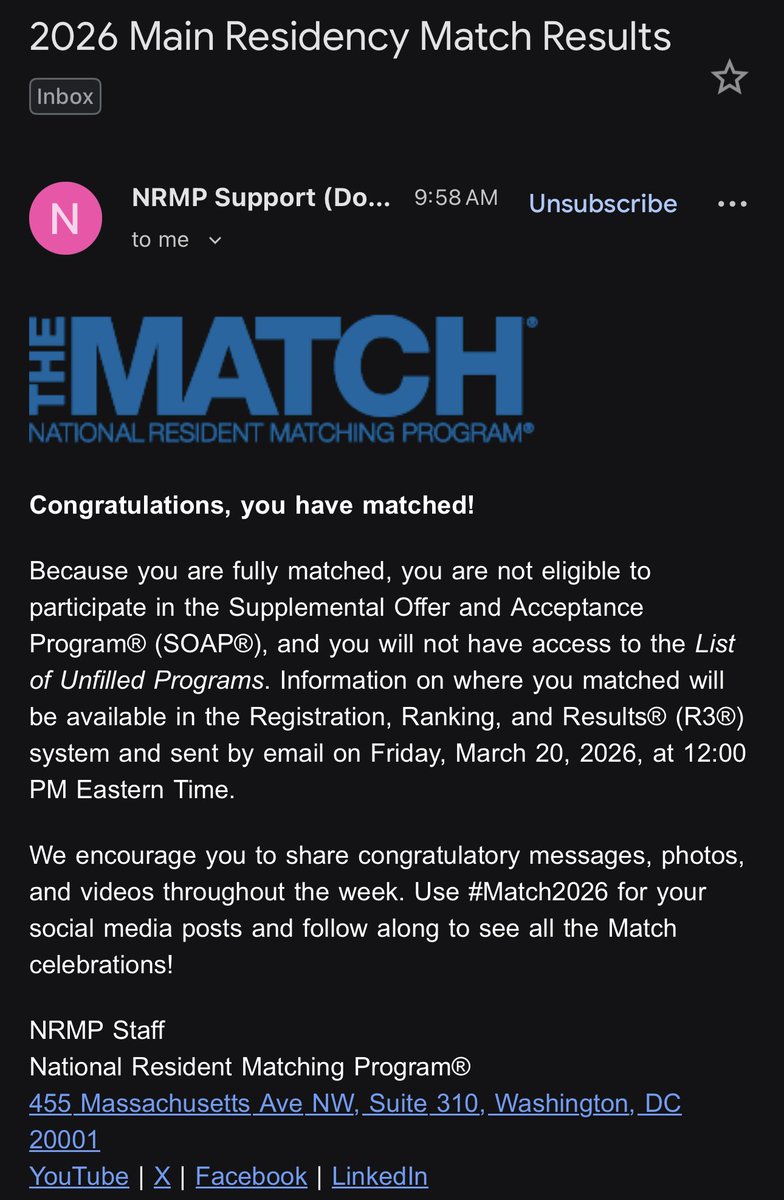
Grateful, humbled and in awe. Alhumdulilah a billion times. Can’t believe it!! But your girl has MATCHEDDDDD ☺️✨#Match2023 #NRMP #MatchDay2023

Columbus, OH 🇺🇸 English
Chanza Shaikh
8.7K posts

@cfshaikh
PGY-3 @LSUHS @LSUHS_IM | Research Fellow @OSUCCC_James | MBBS | 🇵🇰