Javier Pérez Ardavín 已转推

🚀 New paper out!
ARPI intensification in non-metastatic HSPC.
📄 rdcu.be/fcPvR
Congrats to all co-authors 👏
Special thanks to Patricia Willisch & Beatriz Vázquez
#ProstateCancer

English
Javier Pérez Ardavín
822 posts


@jpardavin
Uro-oncología en H. U. i P. La Fe y andrología en Quirón Valencia, FEBU, Doctorando en último año.

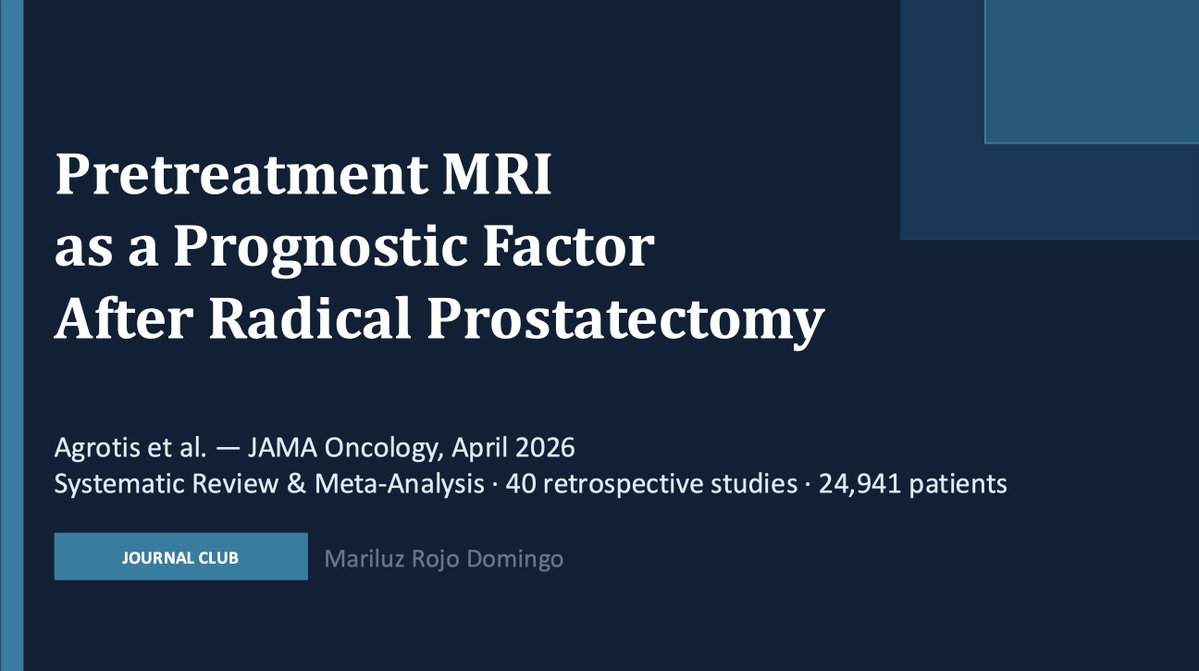
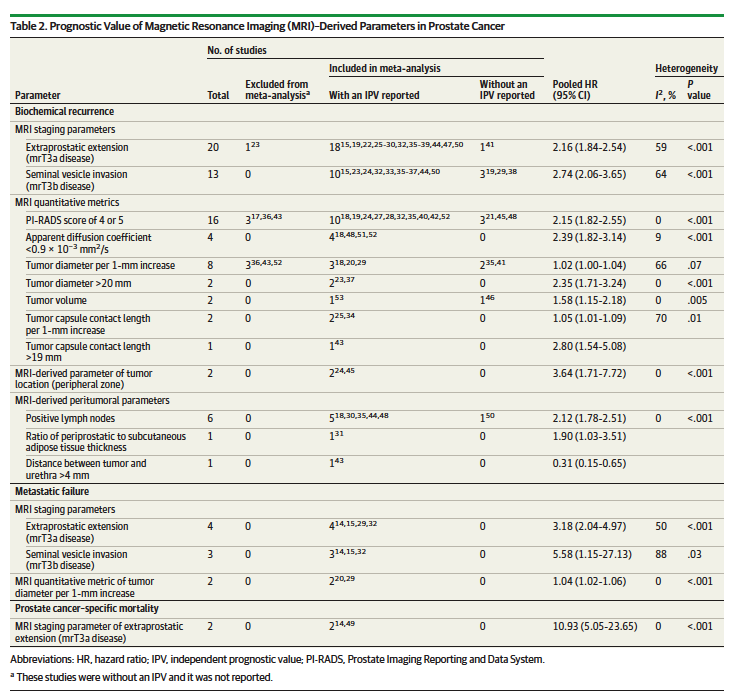
🚨Preop MRI before radical prostatectomy isn't just for surgical planning, it predicts survival.🚨 New meta-analysis (n=24,941) in @JAMAOnc : 🔬 mrT3a (EPE): HR 2.16 for BCR, HR 10.93 for PCSS ⚠️ mrT3b (SVI): HR 2.74 for BCR, HR 5.58 for MFS 📊 PI-RADS 4/5: HR 2.15 for BCR 📏 Tumor >20mm: HR 2.35 for BCR 🌊 Low ADC (<0.9): HR 2.39 for BCR All independent of PSA, Gleason, and pathologic stage. 🧲 Your preop MRI is a prognostic biomarker. Start treating it like one! 🔗shorturl.at/yq3q9 @PCFnews @PCF_Science @UrologyTimes @urotoday













Waiting for @TylerSbrt7 to unpack this in a 🧵 Thanks to the ProtecT trial team, the great pathologists who conducted the review, the OCHRe and CUH Tissue Bank teams who retrieved and digitised slides, and all trial participants @Freddie_Hamdy @Tristan_Radiol @ian263



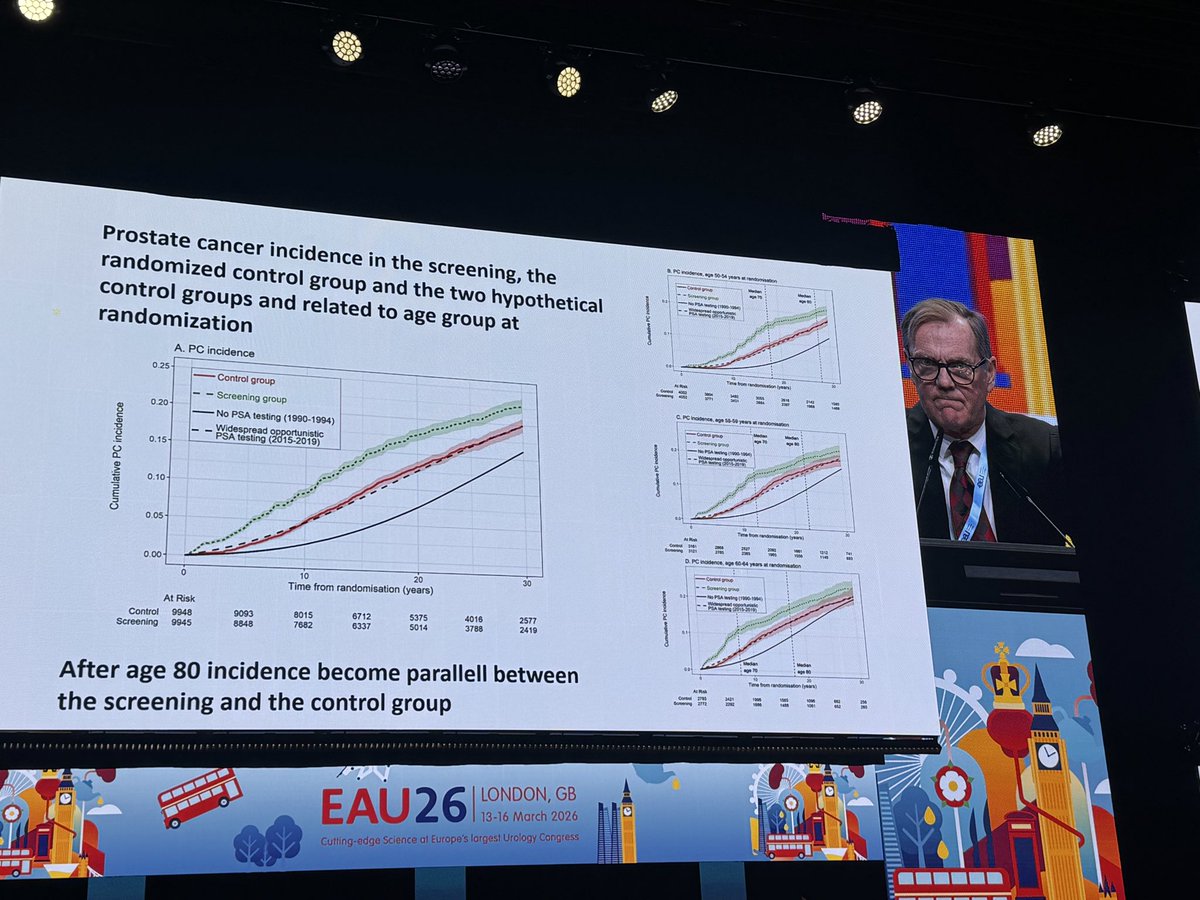
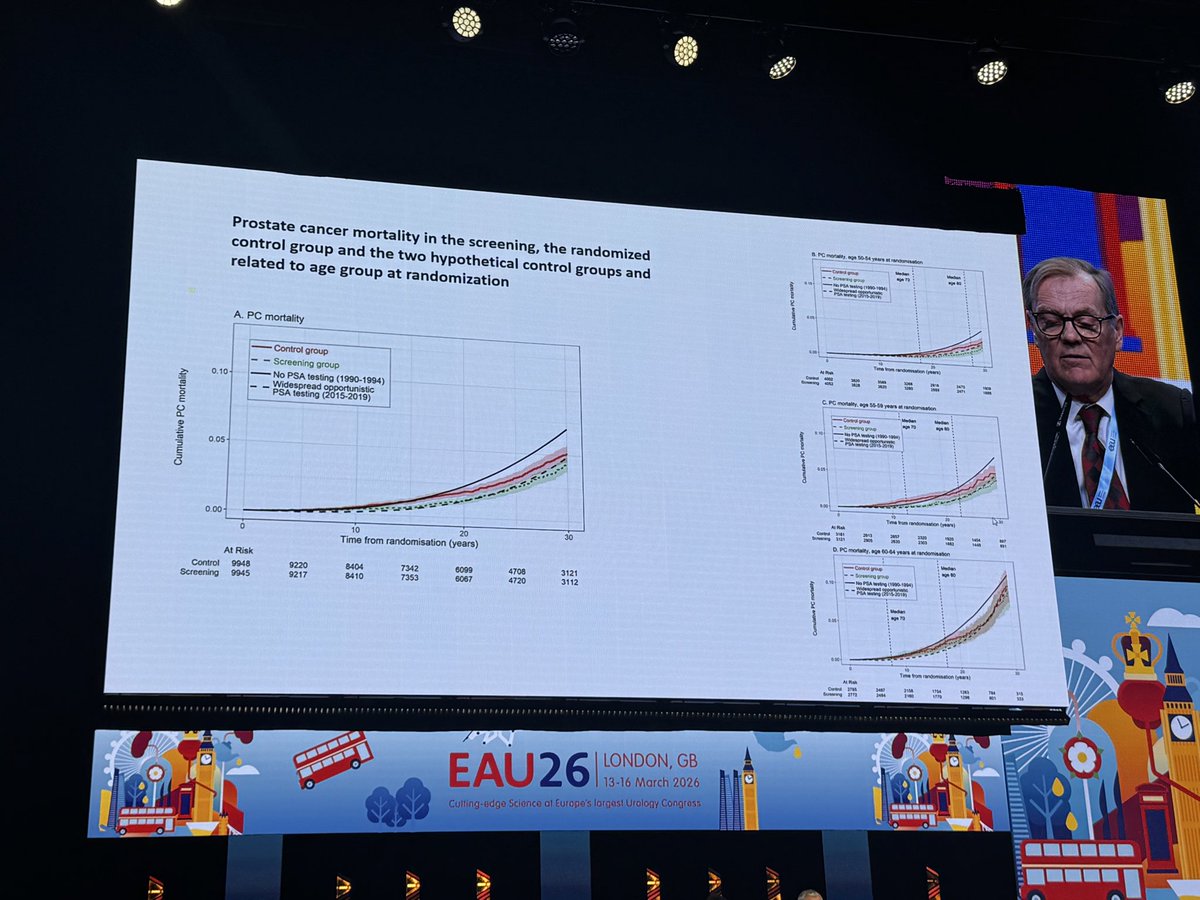
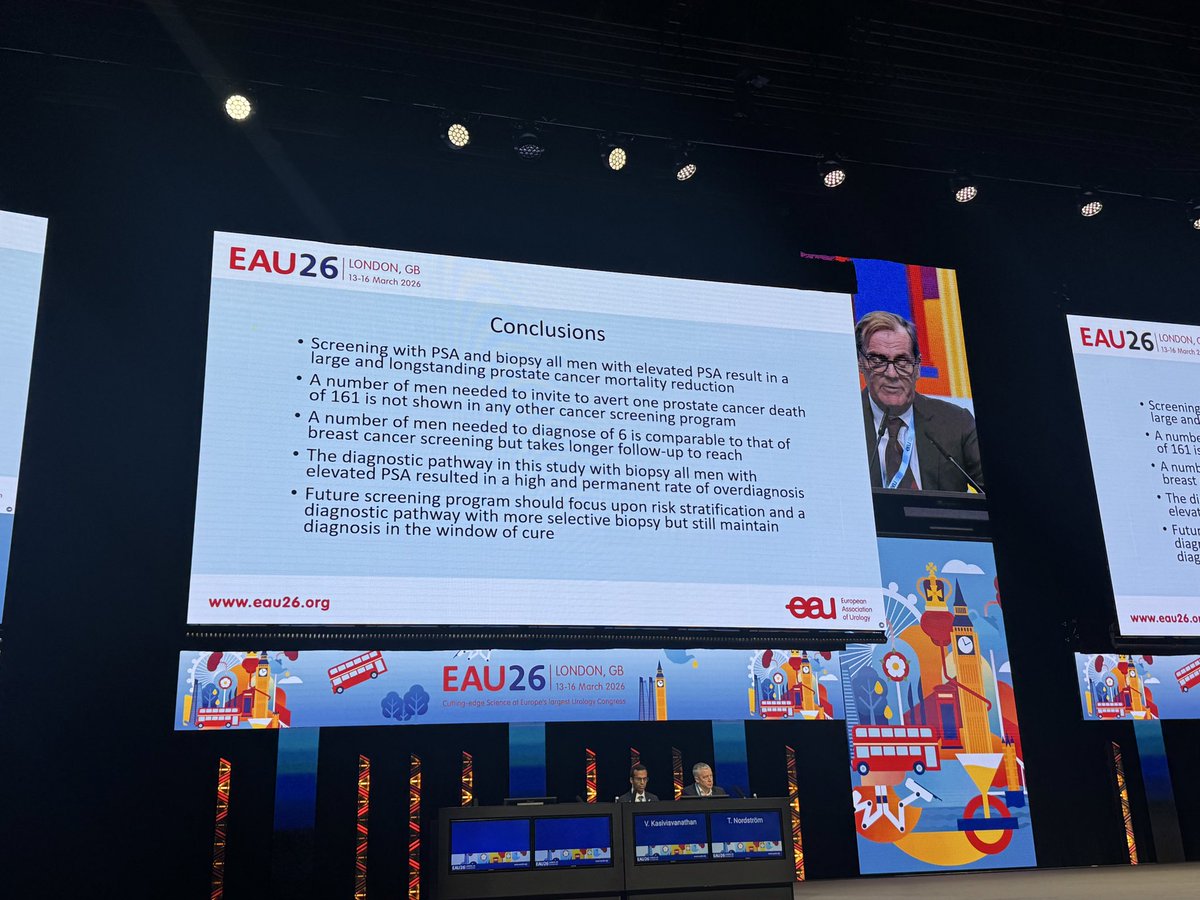
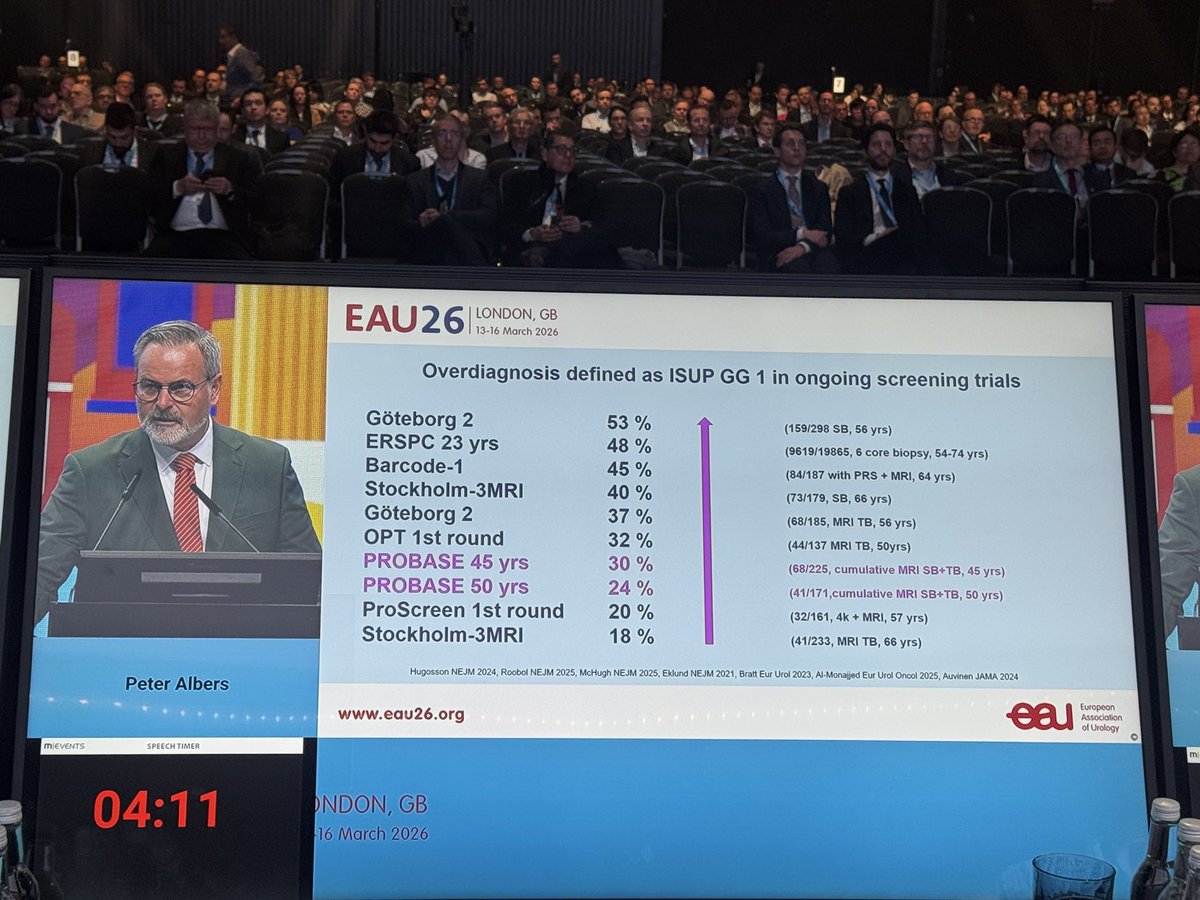
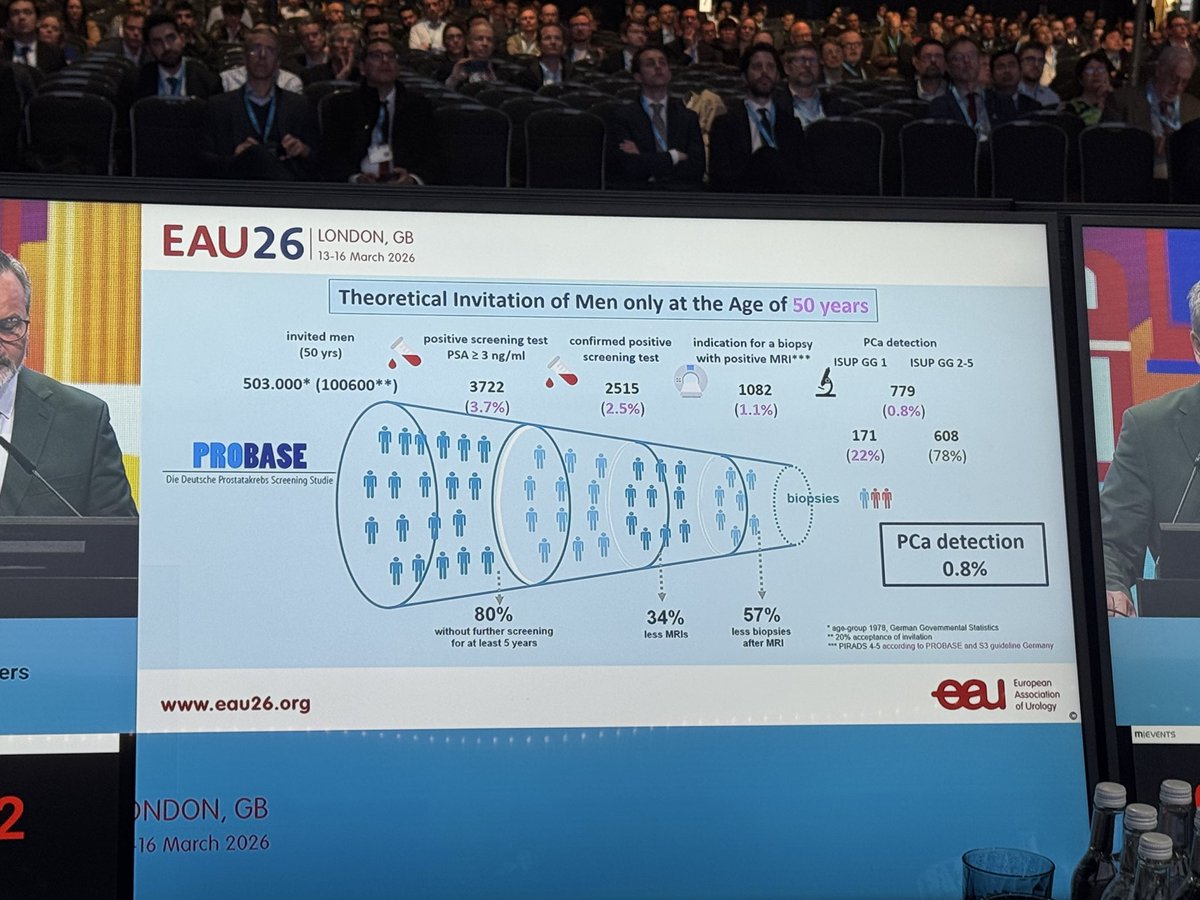
Prof Hugosson: Göteborg trial with 30 year outcomes! NND falls to -6-, with greatest benefit for men 50-59 at randomization. Despite no image guidance, high overdx, and suboptimal tx. Best evidence we have re: the evidence for #prostatecancer screening. Get tested! #eau26 @uroweb