
Anna Vasileva
205 posts
Anna Vasileva
@pathoblog
MD, Surgical Pathologist | Enthusiast in the Education of Junior Pathologists
加入时间 Mart 2020
850 关注858 粉丝

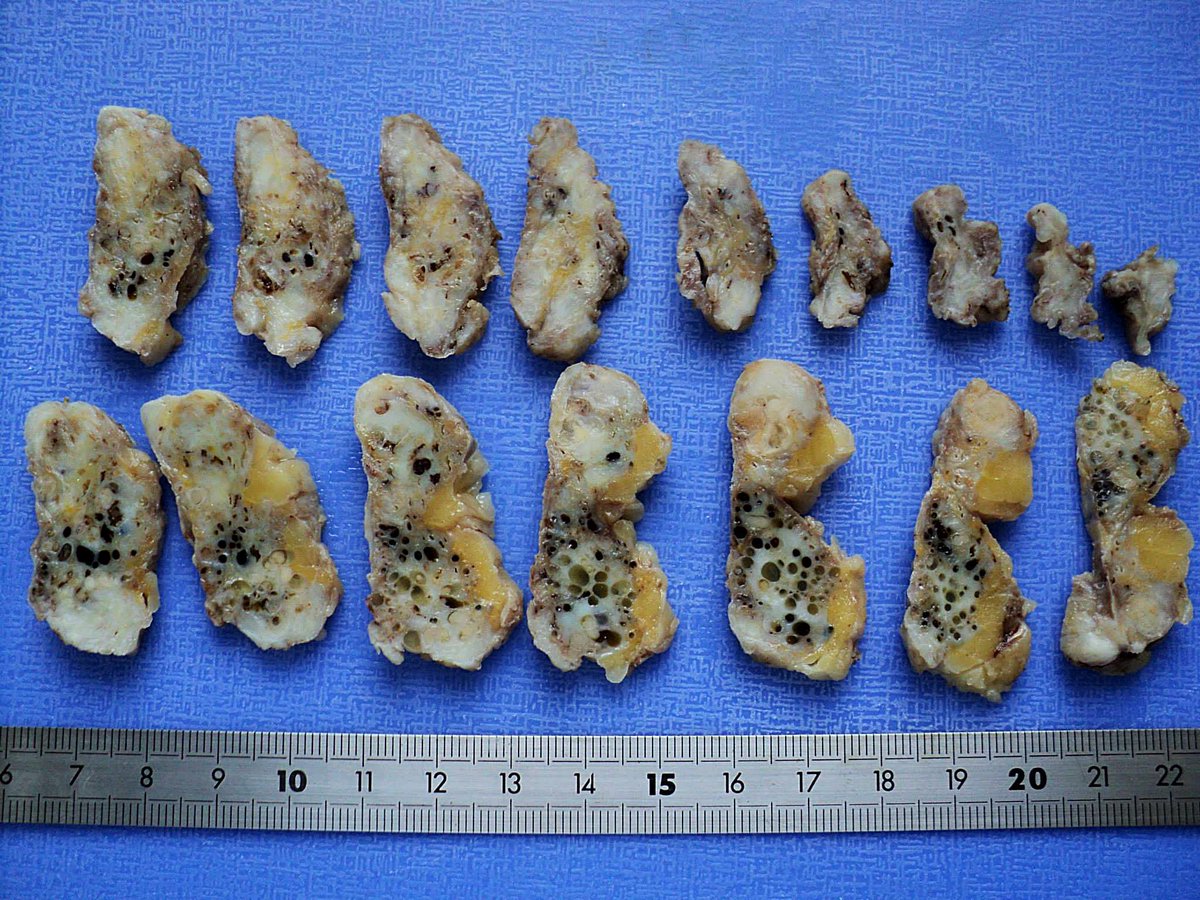
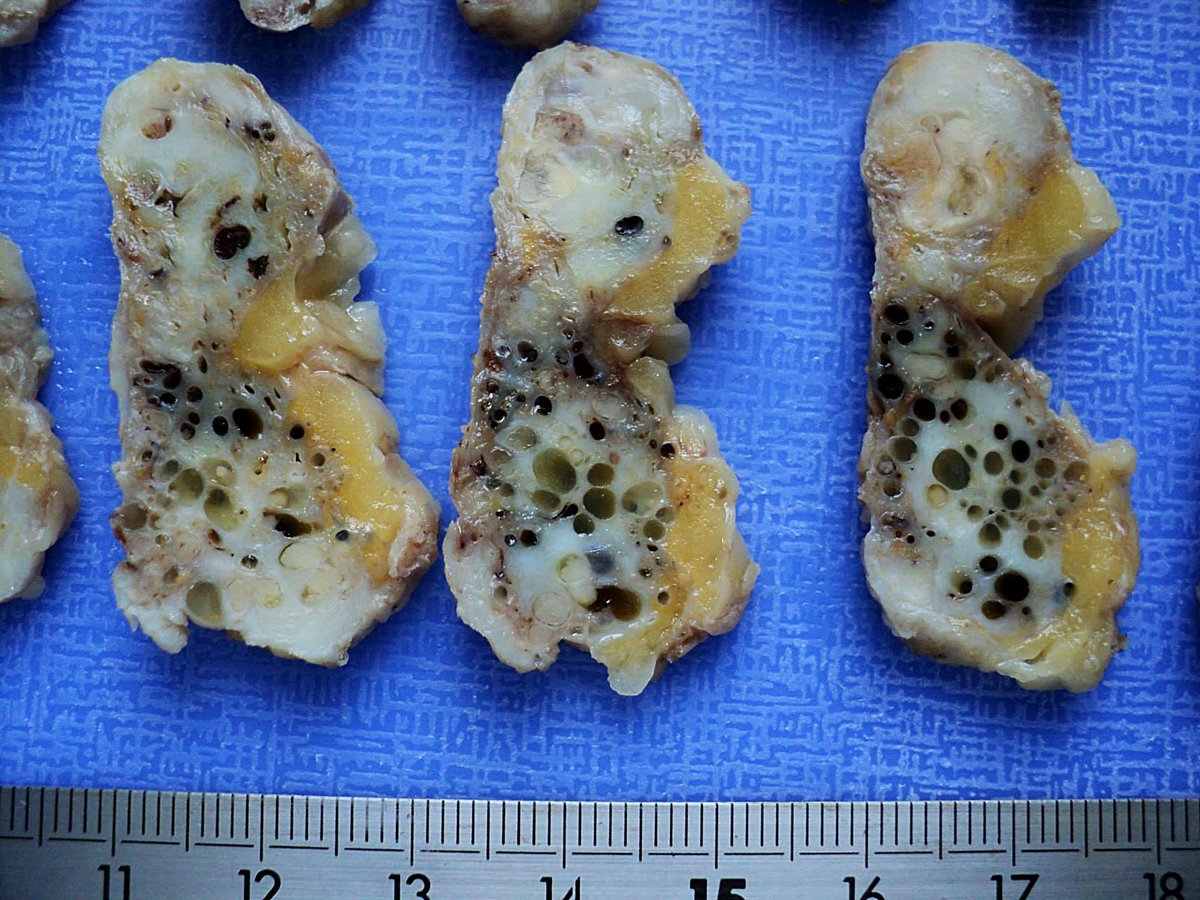
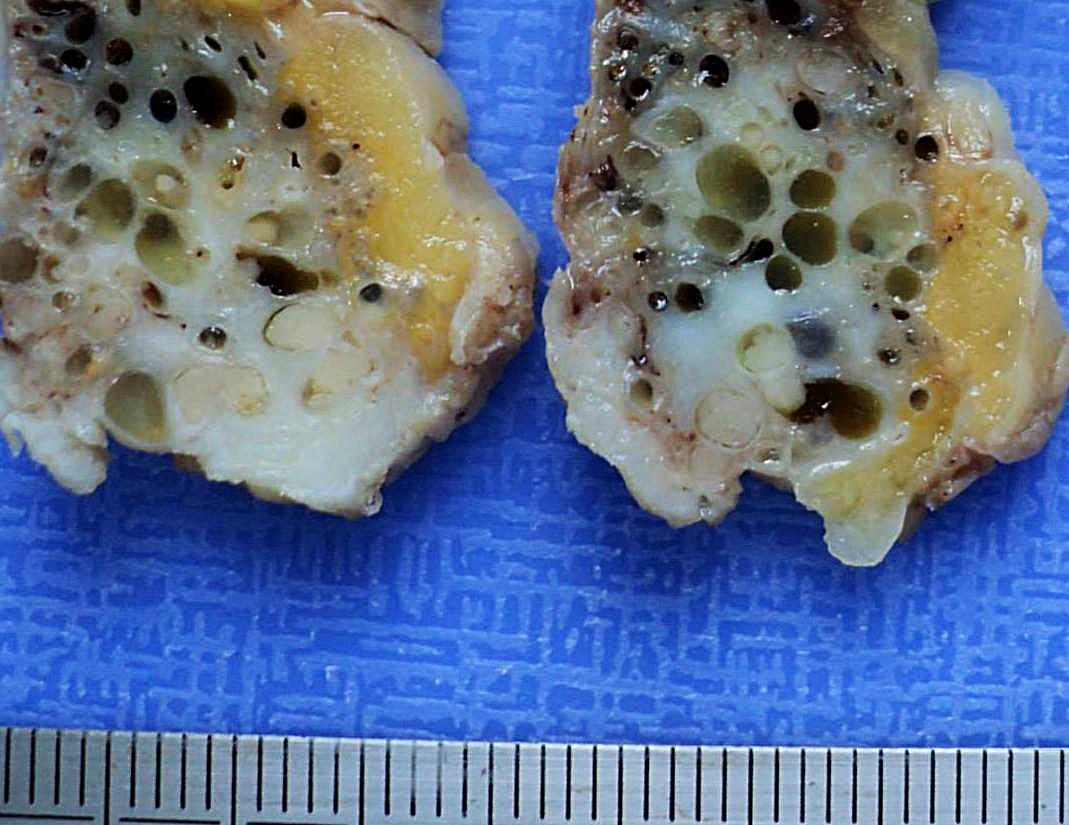
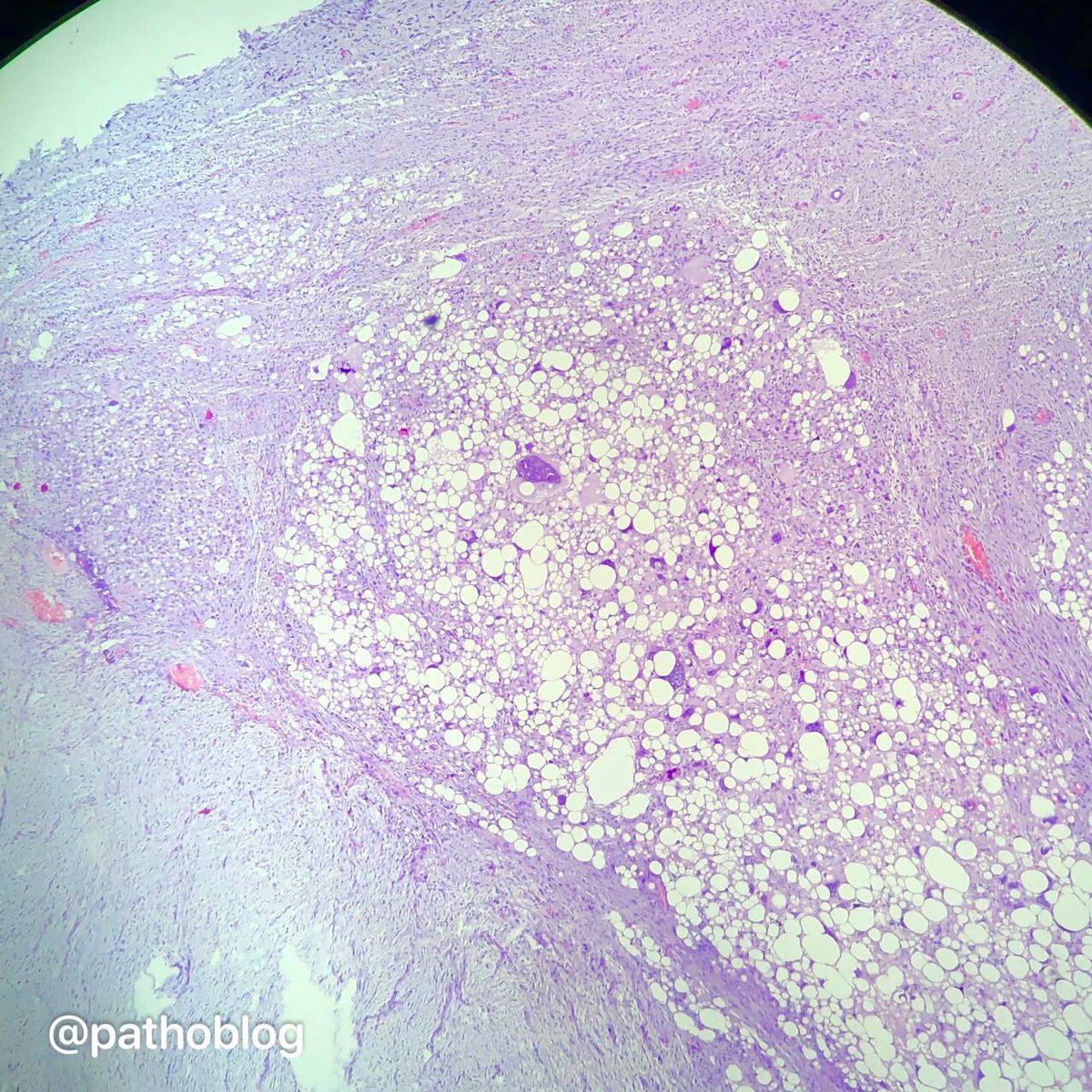
F62, omentum with subtotal metastatic lesion.
#Grosspath #GUpath #pathtwitter #pathology
When the topic of the omentum hit the popular Twitter trends, I remembered my photos from the folder ‘serous ovarian carcinoma, HG’ 🙃


English
Anna Vasileva 已转推

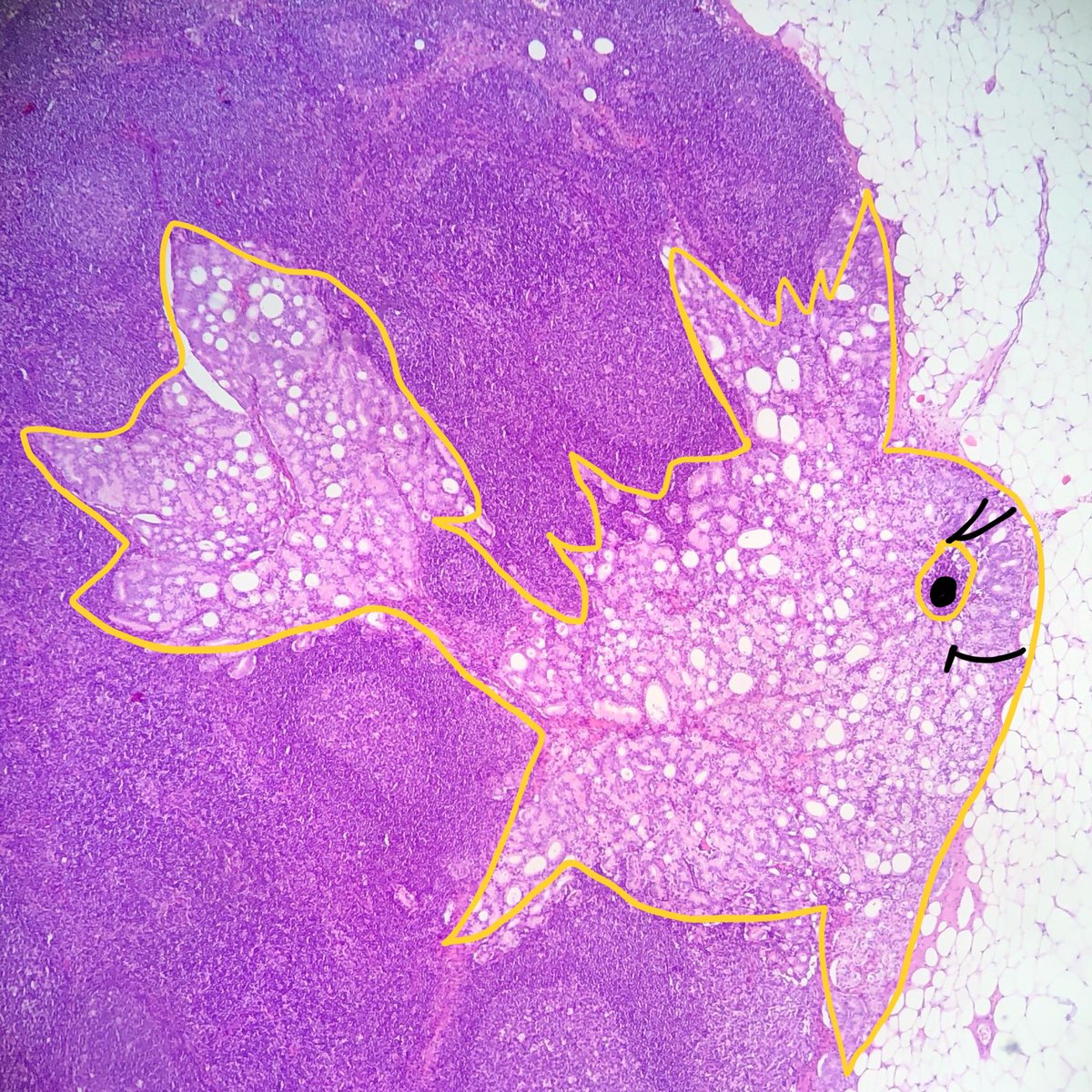
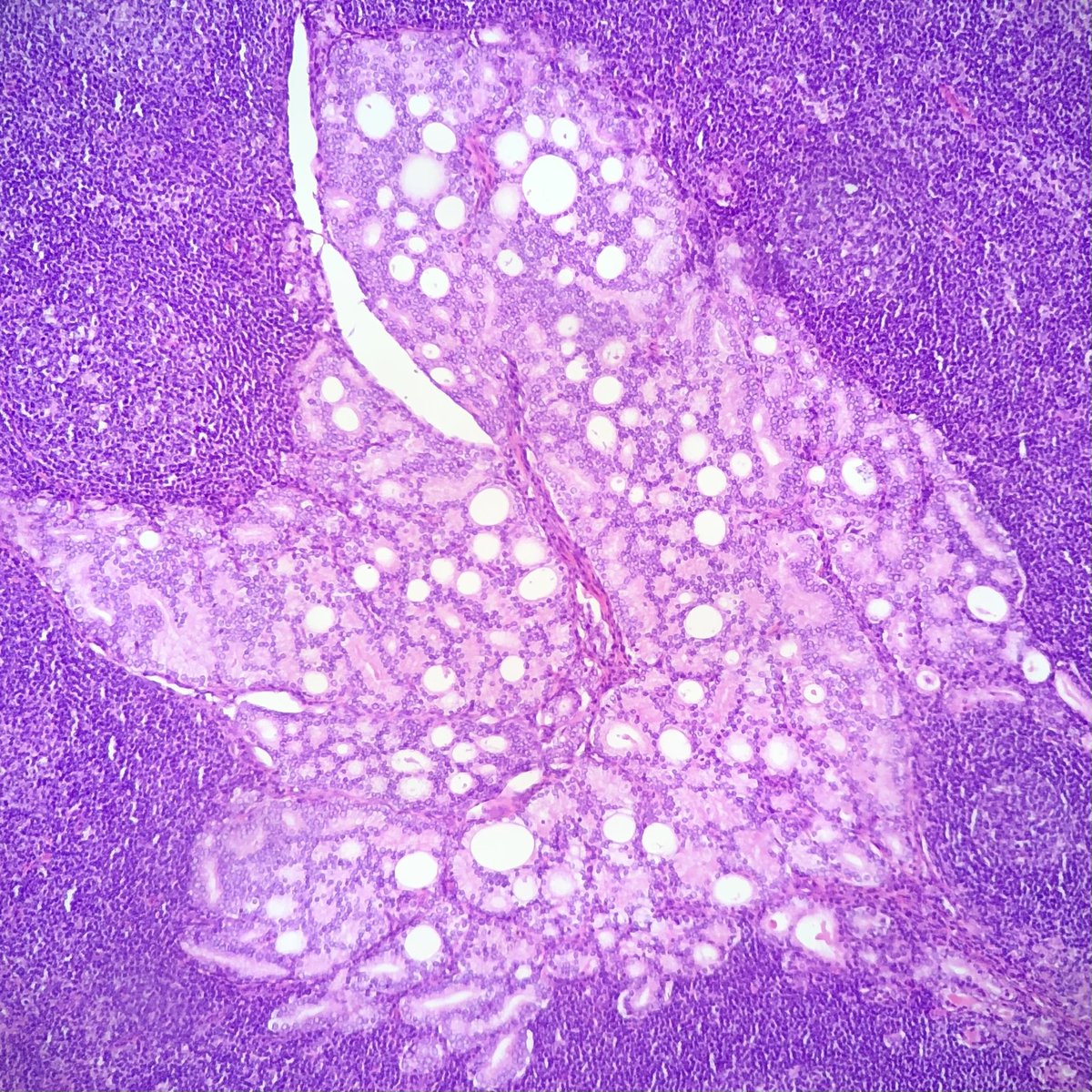
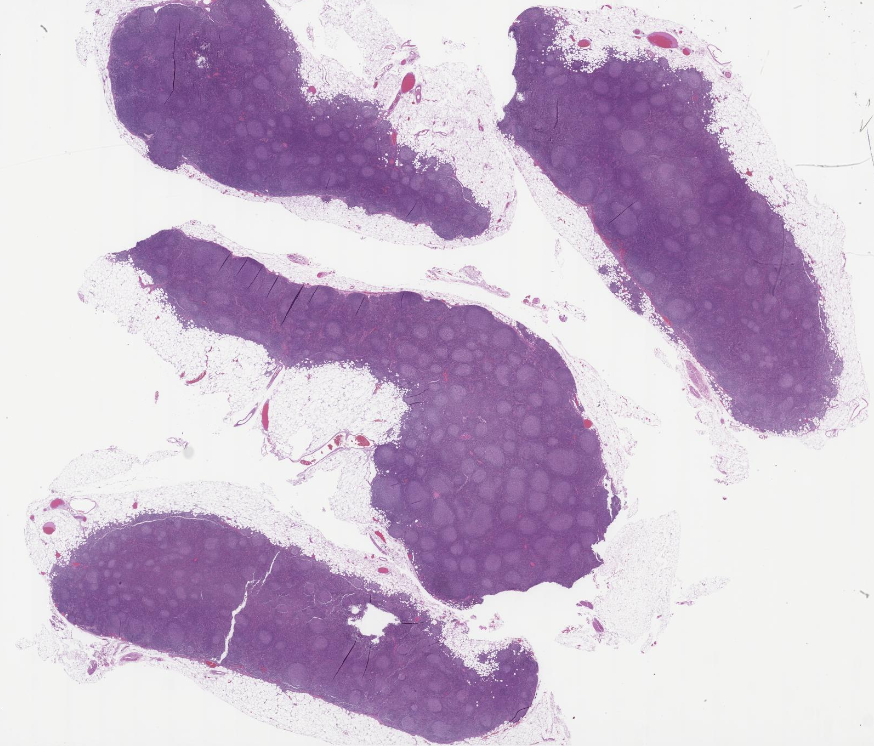
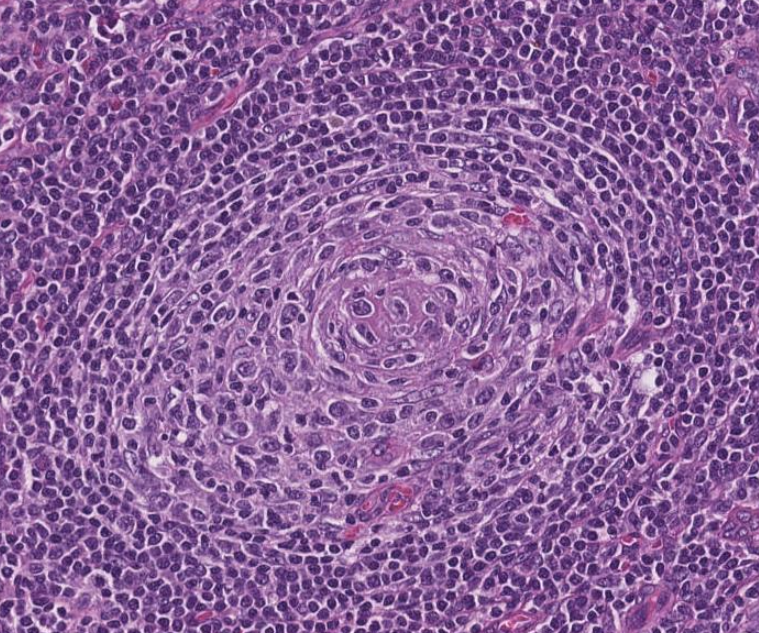
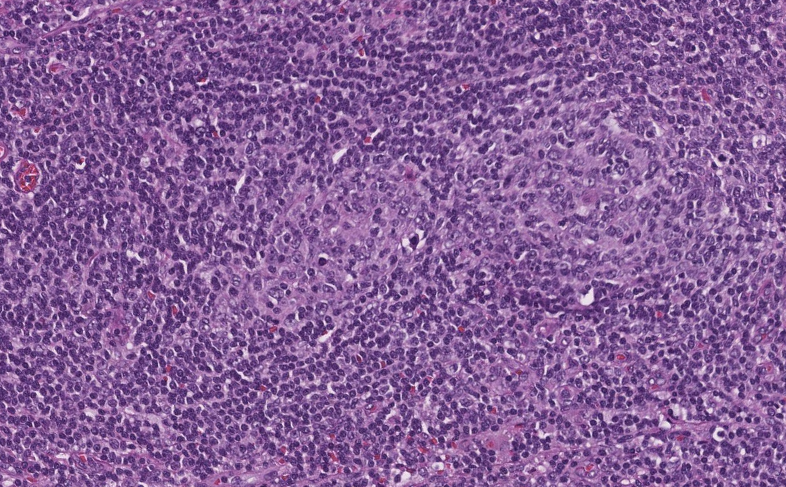
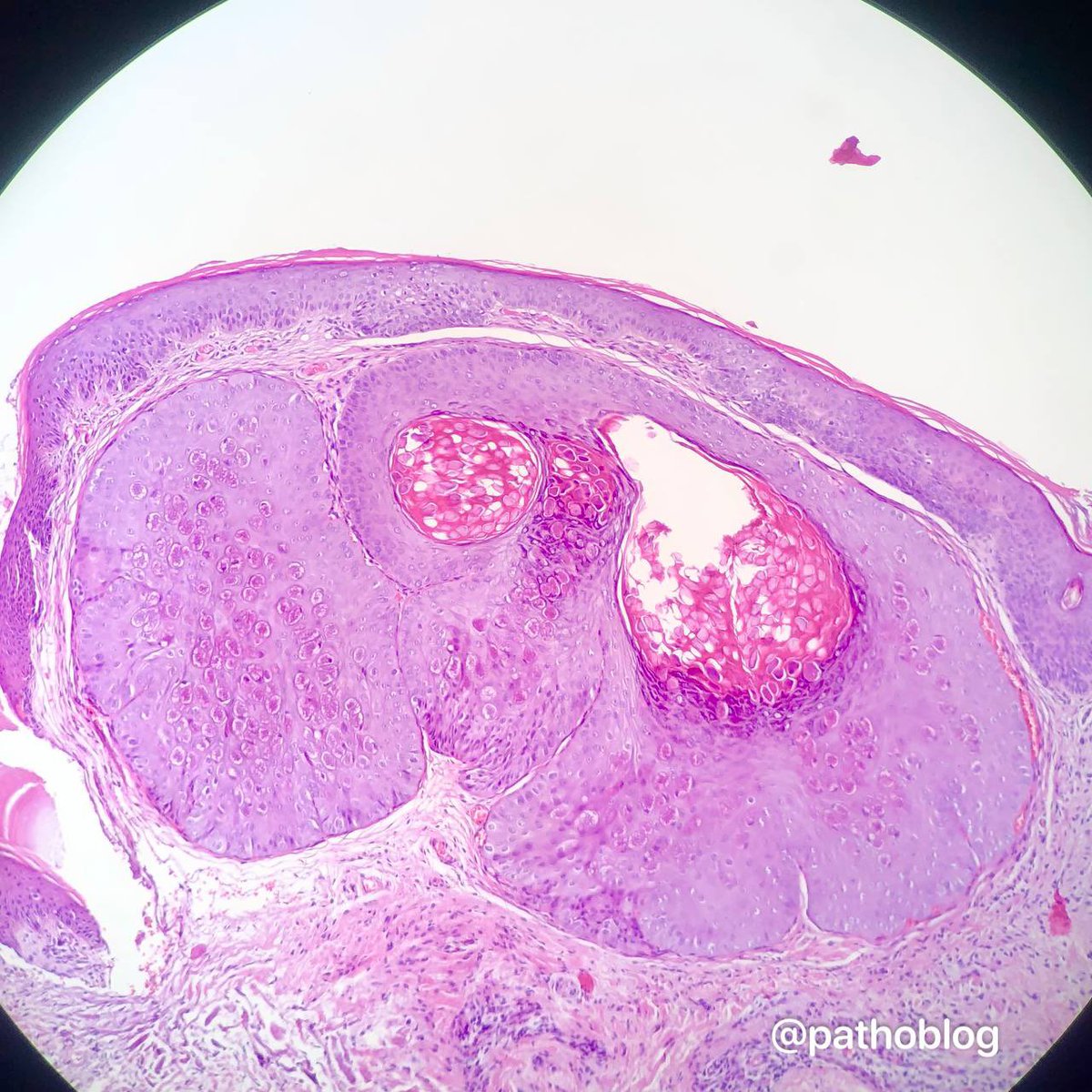
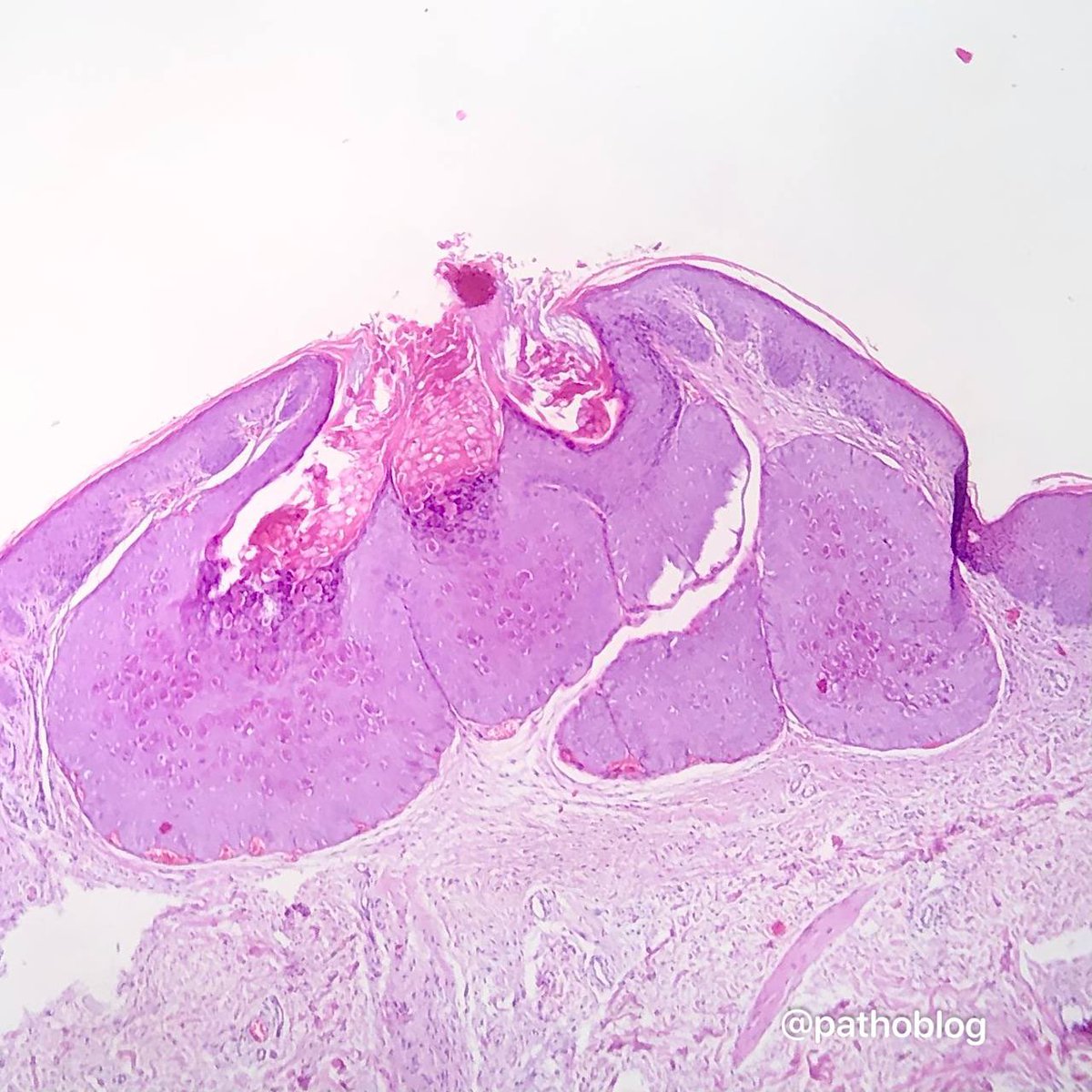
Illustration of a case of Follicular Lymphoma with Hyaline Vascular Unicentric Castleman Disease-"like" changes➡️
🩸Depleted germinal centers (Fig 2)
🩸Onion-skinning of mantle zones (Fig 2-3)
🩸Penetrating hyalinized vessels, imparting a lollipop-like configuration of germinal centers (Fig 3)
🩸Twinning (fusion) of follicles (Fig 4)
This case turned out to be postive for BCL2 translocation by FISH, with an aberrant CD10-positive population by flow cytometry analysis.
More on this variant of Follicular Lymphoma➡️pubmed.ncbi.nlm.nih.gov/28873356/
To complicate things, the "follicular variant" of Hyaline Vascular Unicentric Castleman Disease, with characteristic back-to-back follicular architecture, may greatly mimic follicular lymphoma as well ➡️pubmed.ncbi.nlm.nih.gov/8116226/
➡️pubmed.ncbi.nlm.nih.gov/19039195/
In summary, by morphologic examination, Follicular Lymphoma may present like Hyaline Vascular Unicentric Castleman Disease; Conversly, Hyaline Vascular Unicentric Castleman Disease may show a presentation very similar to Follicular Lymphoma
#hemepath #lymsm #PathX #PathTwitter #MedX #MedTwitter #MedEd

English
Anna Vasileva 已转推

Breast, Fibrocystic Changes, Multiples Intraductal Papillomas, Gross pics, #pathology, #pathologists
English
Anna Vasileva 已转推

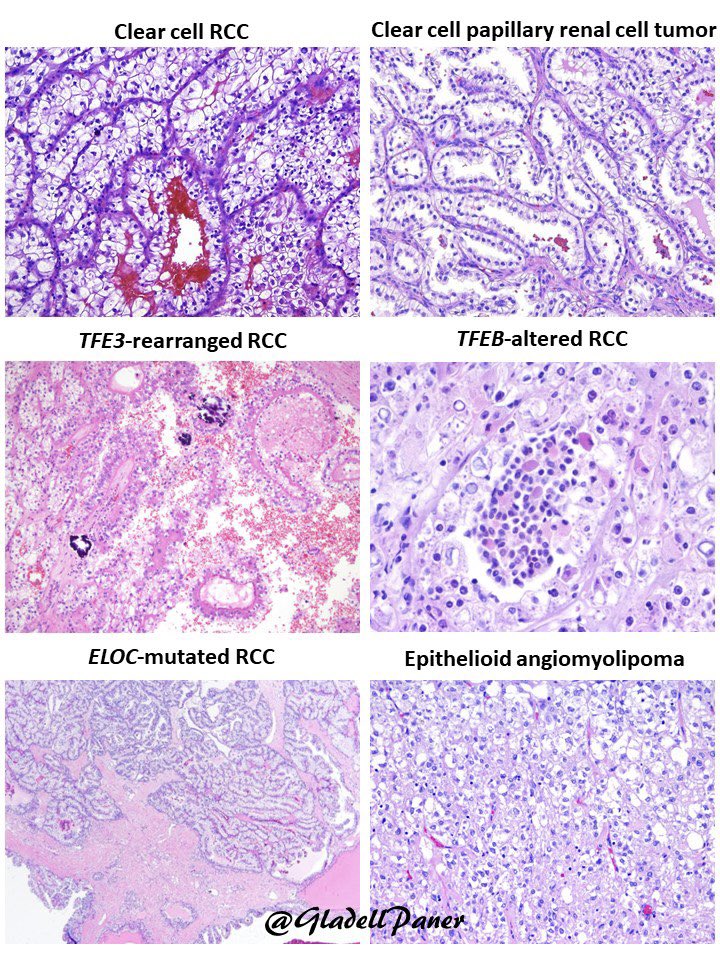
For our 2023 #pathology trainees, remember this #GUPath adage👇
“Not all renal tumors with clear cells are clear cell renal cell carcinoma”
… spot on in this molecular era!
👇Below are DDX for Clear cell #RCC including #renal tumors with some degree of cytoplasmic clearing🔬
English
Anna Vasileva 已转推
Tenosynovial Giant cell tumor
Arises from synovium (joints; bursae; tendon sheath)
Due to CSF1 mutation
Localized type usually on the fingers
Treatment of localized: surgical excision
#pathtwitter #pathsig #orthotwitter #medtwitter #MedStudentTwitter #softtissue


English
Anna Vasileva 已转推
Targeted therapies for colorectal cancer have advanced greatly since my last review on this subject in 2016 with the incomparable @JLHornick. MMR deficiency, high TMB, BRAF, HER2 and numerous rearrangements have all become targetable.

English
Anna Vasileva 已转推
Classic example of collagenous micronodules (aka mucinous fibroplasia) in #prostatecancer #GUPath #pathologists @Pathologists
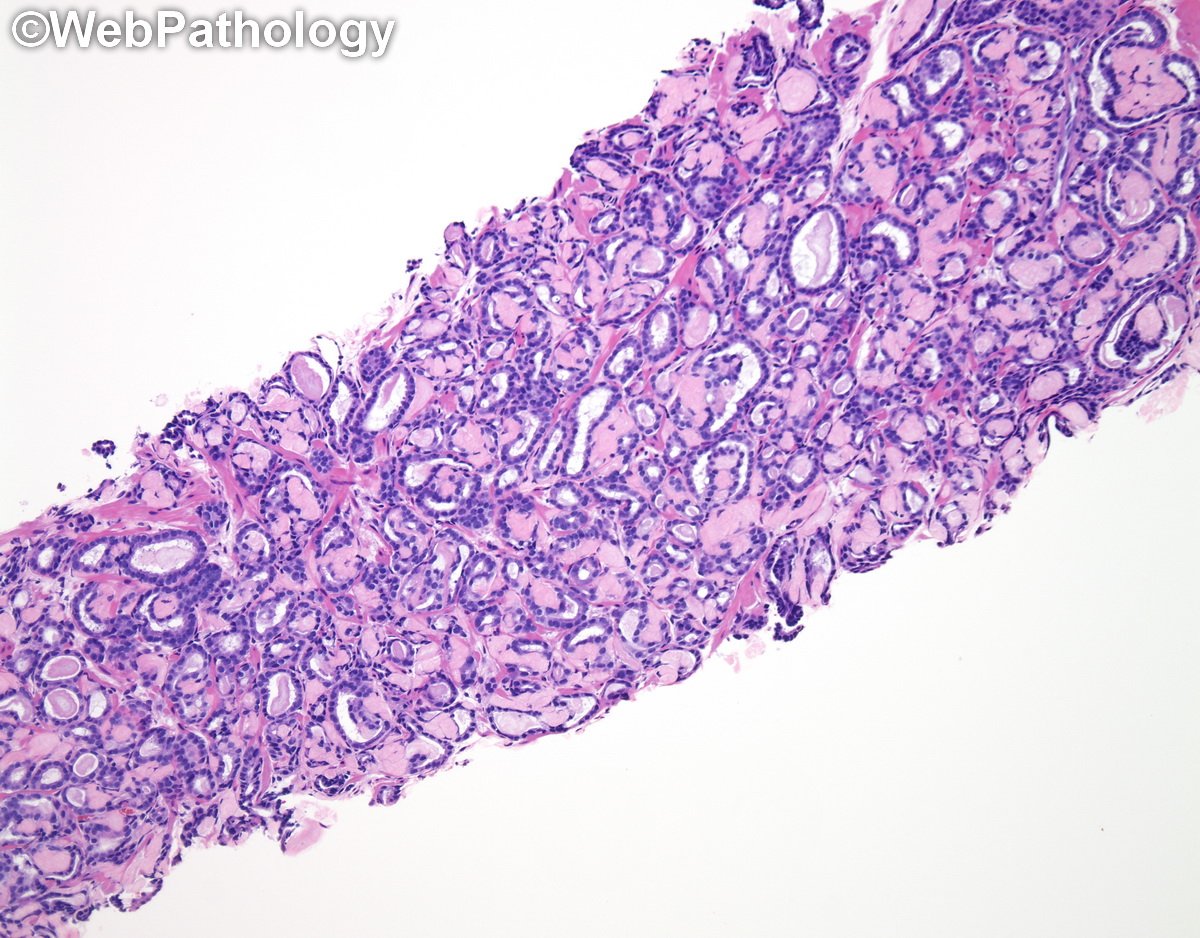

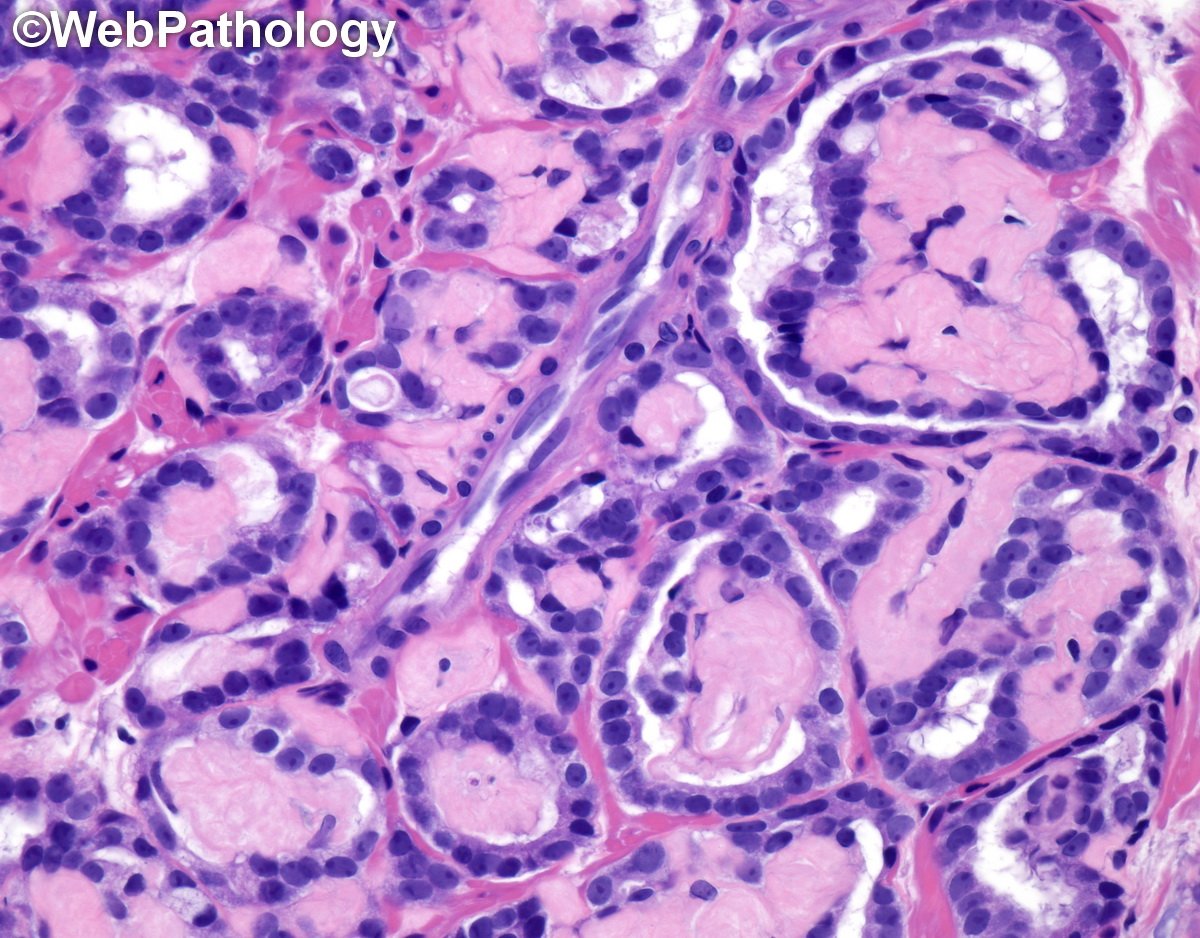
English
Anna Vasileva 已转推
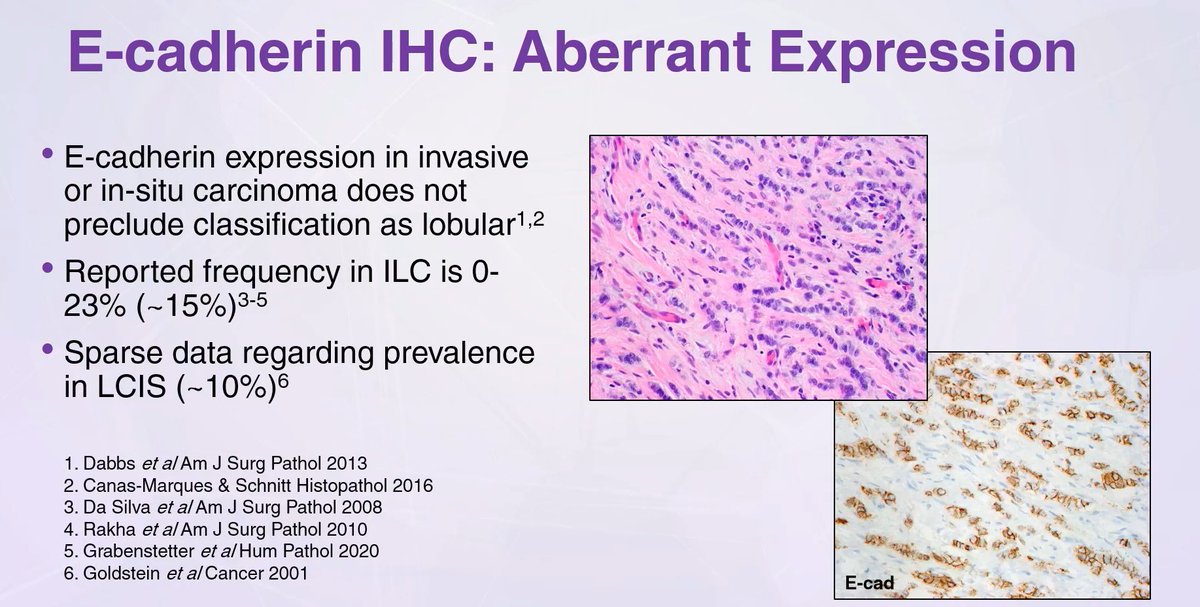
E-cadherin expression in invasive or in-situ carcinoma DOES NOT preclude classification as lobular
Dr, Harrison #USCAP2023 #everydaybreast #breastpath #pathology #pathtwitter #pathologist #pathology #pathresidents
English
Anna Vasileva 已转推
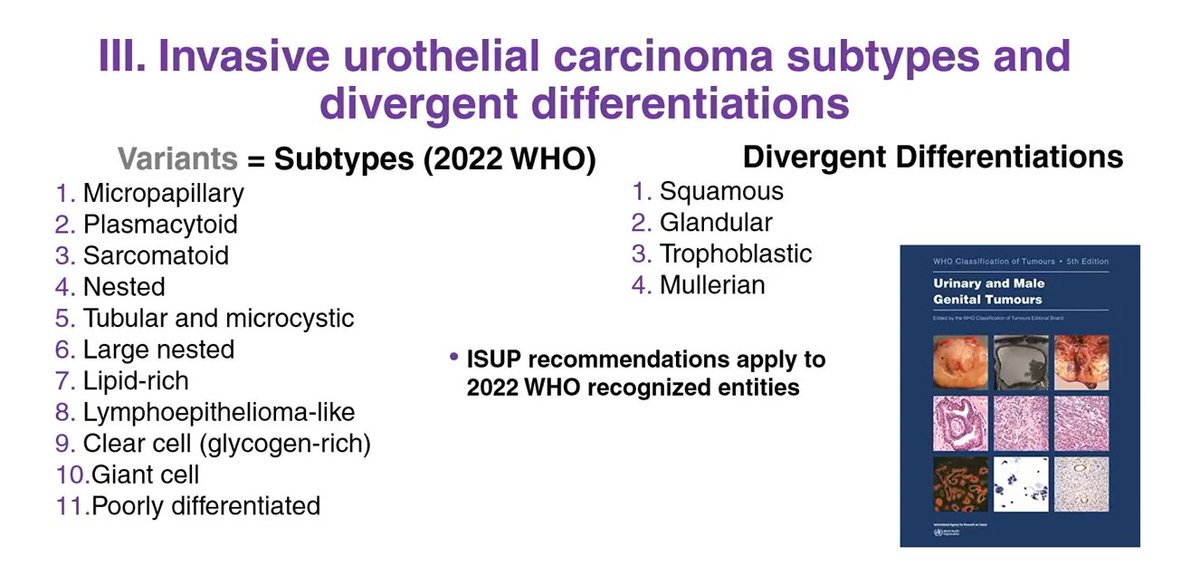
Bladder
Histological subtypes of urothelial carcinoma and those with divergent differentiation are all considered high-grade tumors-WHO 5th edition
Dr. Paner USCAP23 #USCAP2023 #PathTwitter #GUpath #pathology #pathologist #pathresident #pathfellow
English

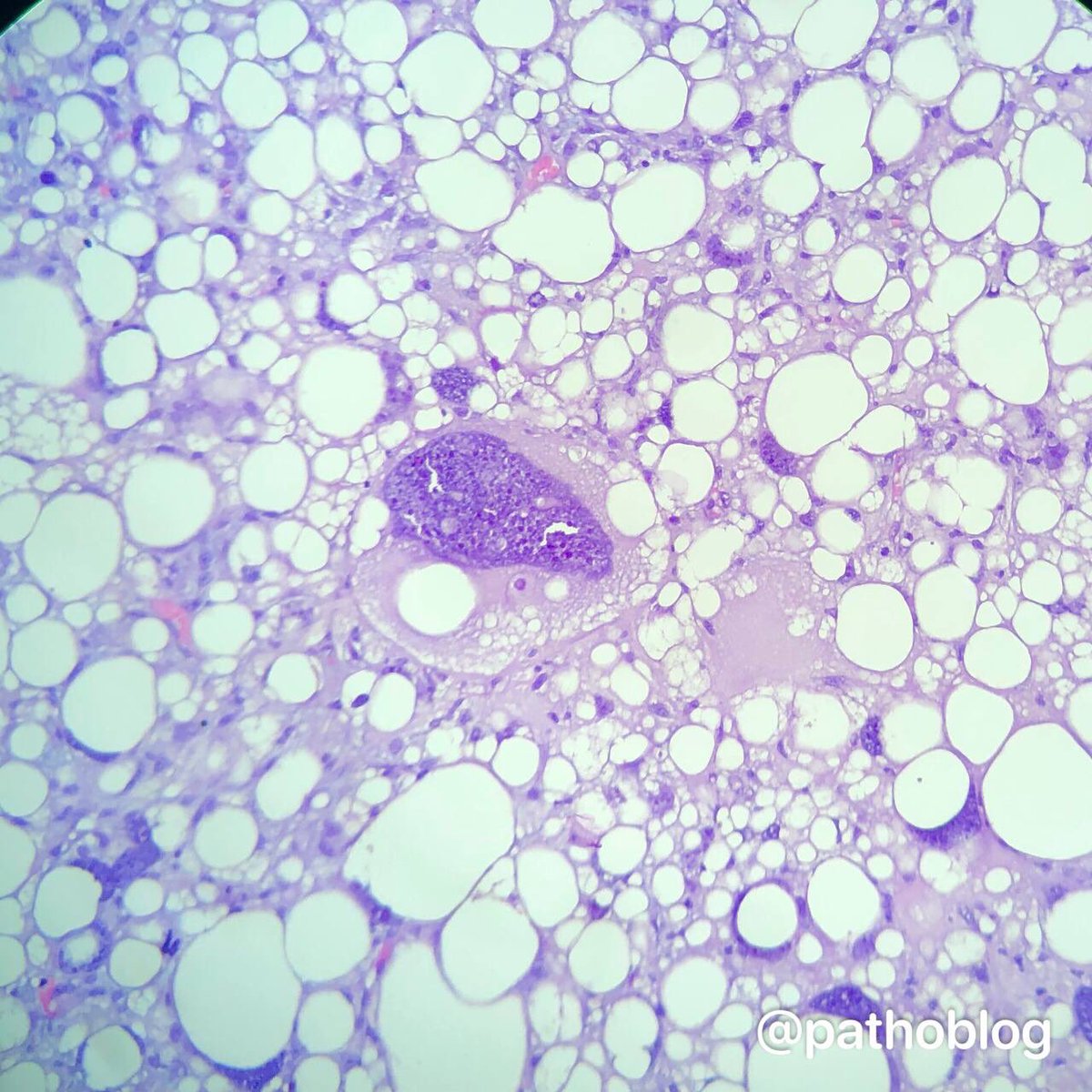
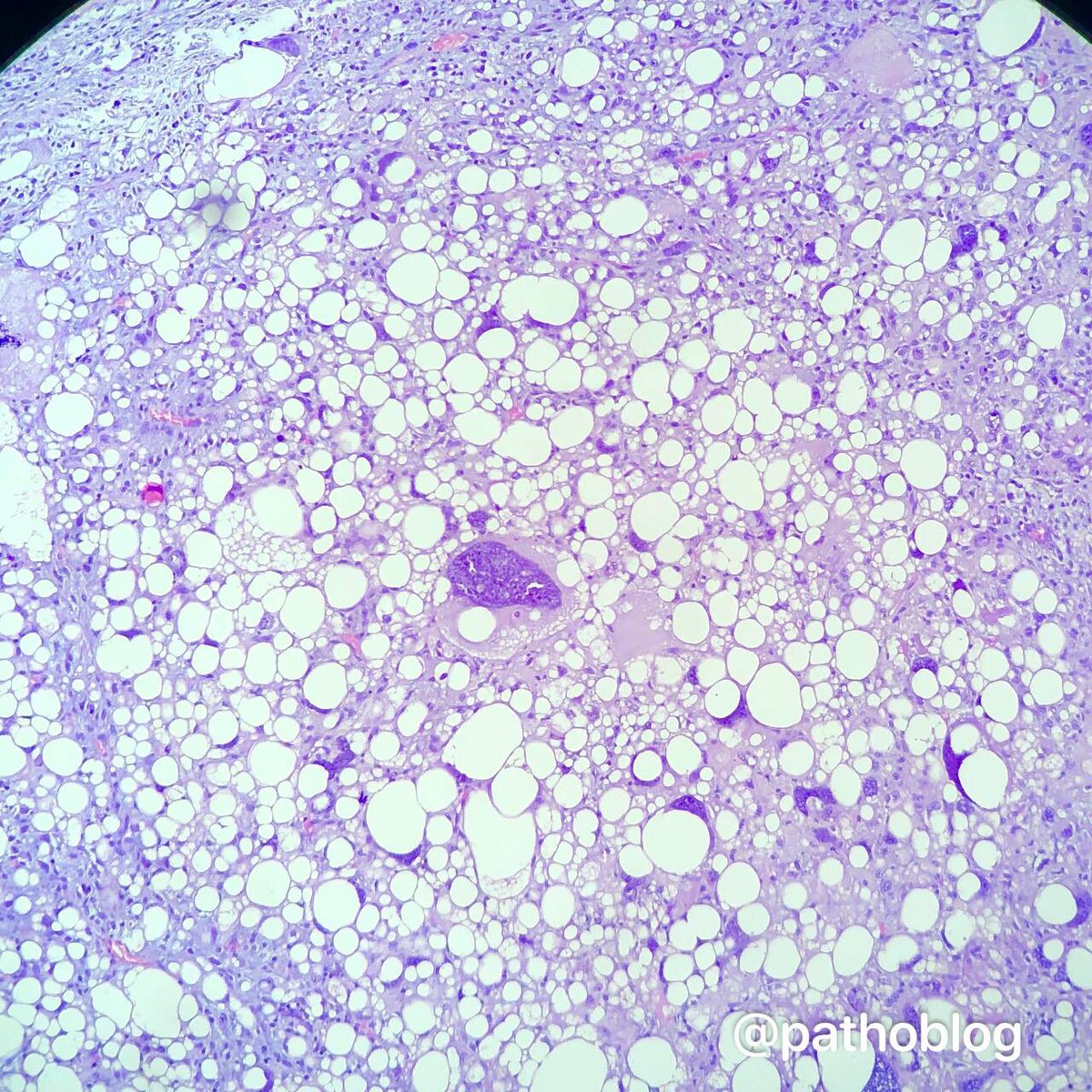
Phyllodes tumor of the breast with liposarcoma. Beautiful bizarre cells! 👻 #pathtwitter #breastpath

English

@atman_ci I’m very glad that the case turned out to be educational! Thanks for sharing 🙏🏻
English
Anna Vasileva 已转推
One in a million Monday.
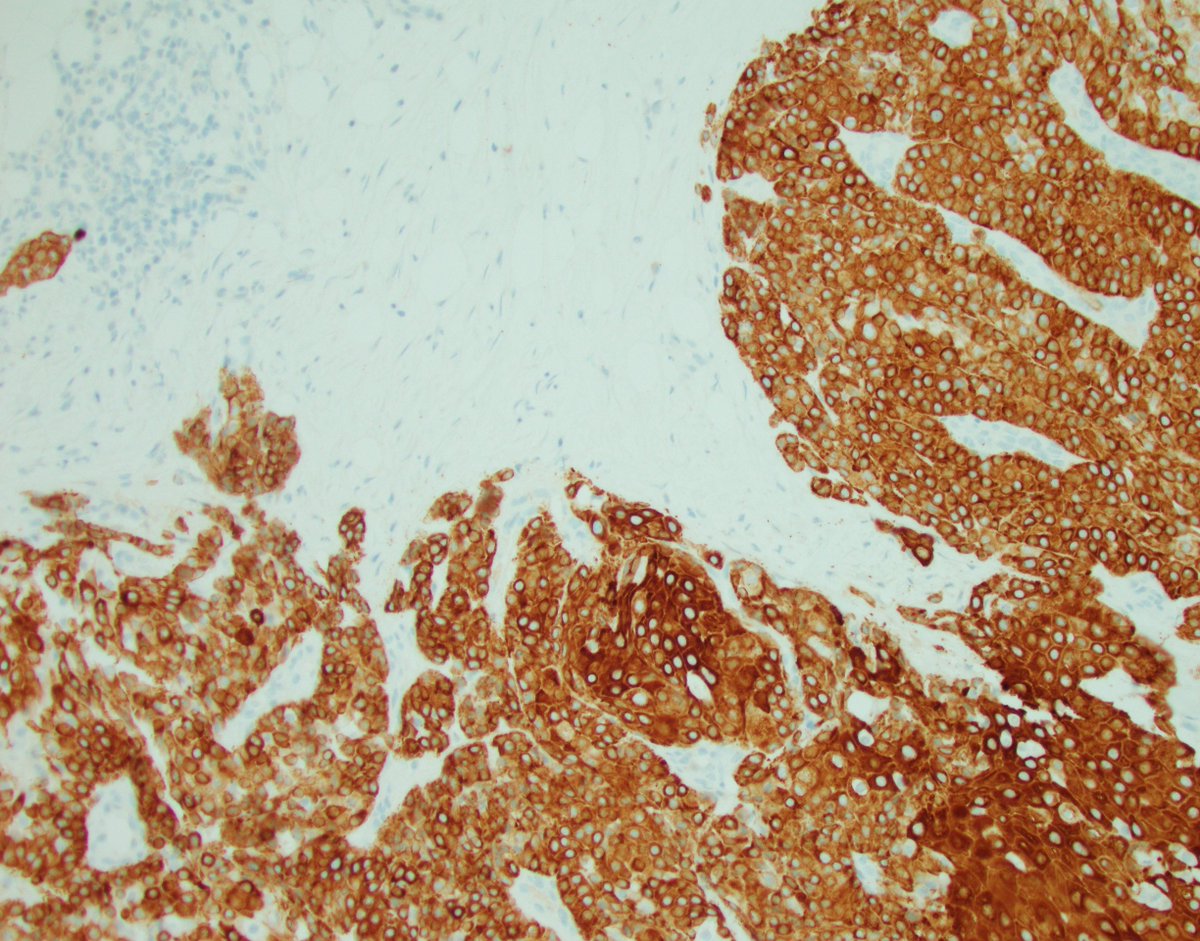
Unwittingly saved by the clinician. This case was not a consult, it was just a good old biopsy from a satellite hospital for whose patients we provide pathology diagnostic services. In that hospital, breast surgeons coordinate breast patient care, perform biopsies, discuss treatment and surgical plans with patients, and eventually refer to oncology as needed. Unlike our radiologists and oncologists here at WashU, the surgeons at that hospital do not want to get a tumor diagnosis then get an addendum with the biomarkers. They like to see a complete report all at once. I can't say I dislike that practice, and after this particular case, I like it even more, because it saved me from a major (albeit exceptionally rare) misdiagnosis.
The images below depict a tumor I was squarely going to call invasive solid papillary carcinoma because, to my eyes, that's exactly what it looks like. Except that's not what it is. And because I waited for the biomarkers to sign it out, I was fortunate to find out it was triple negative, which would be extremely unusual for solid papillary carcinoma. So, I contacted the surgeon and dug into her chart, and sure enough, the patient had a history of metastatic mucoepidermoid carcinoma of the minor salivary glands. That's when I started seeing a hint of squamous differentiation and possible mucous cells. CK5/6 and p63 were done and were confirmatory. MAML2 FISH was also positive and sealed the deal. I did not find a similar case in the literature.
Lessons from this monumental near miss.
1. Clinician preferences did save me this time, but the clinician's omission of pertinent medical history is a common and persistent problem.
2. Always remember that breast biomarkers are not only predicitve and prognostic, but also diagnostic. If their pattern does not fit with the tumor's morphology, take a deep breath and dive into those muddy diagnostic waters.
3. Again and again, be vigilant, look for clinical information, don't make assumptions. Easier said than done, of course, and I do not want to encourage paranoia because I am not the paranoid type, but sharp alertness is one absolute must, and not allowing hasty explanations for things that don't quite fit is another.
4. Morphology is key, but nature loves mimicry. Don't be a hammer. Everything is not a nail.
@washupathedu @wusm_pathology #PathTwitter #Breastpath #ENTpath



English


Anna Vasileva 已转推
High yield 💎appendiceal lesions.
- Difference between diverticula and LAMN
#surgpath #pathology #PathTwitter #GIpath
Check it online 📱digital.olivesoftware.com/olive/odn/capt…
Thanks for sharing @Voltaggiol 🌟


English
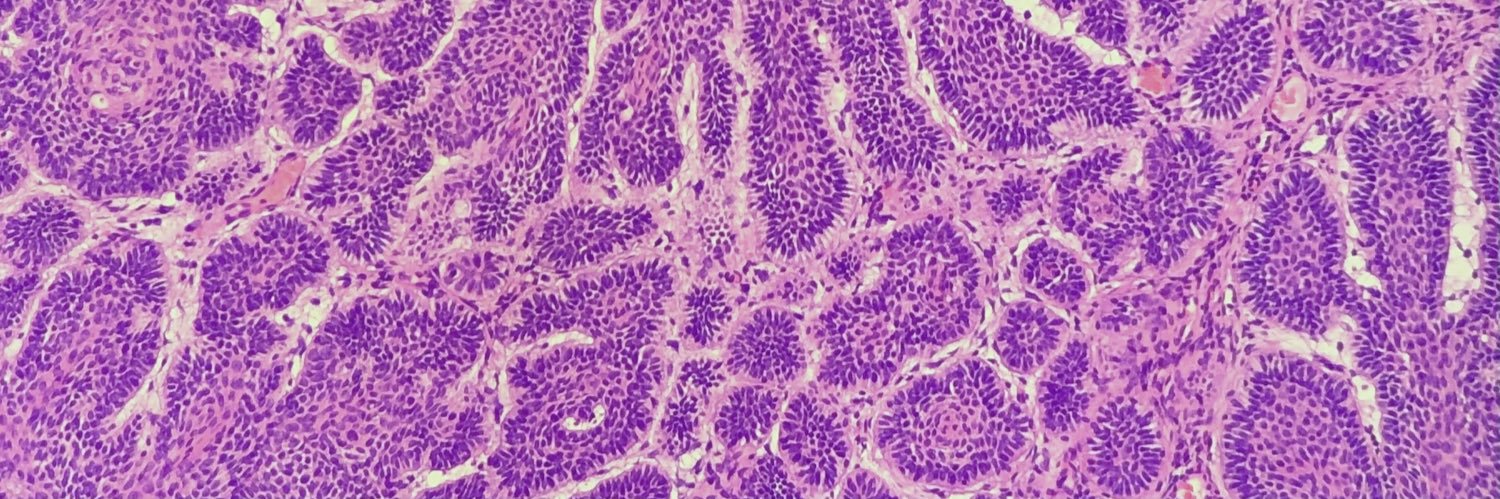
Anna Vasileva 已转推
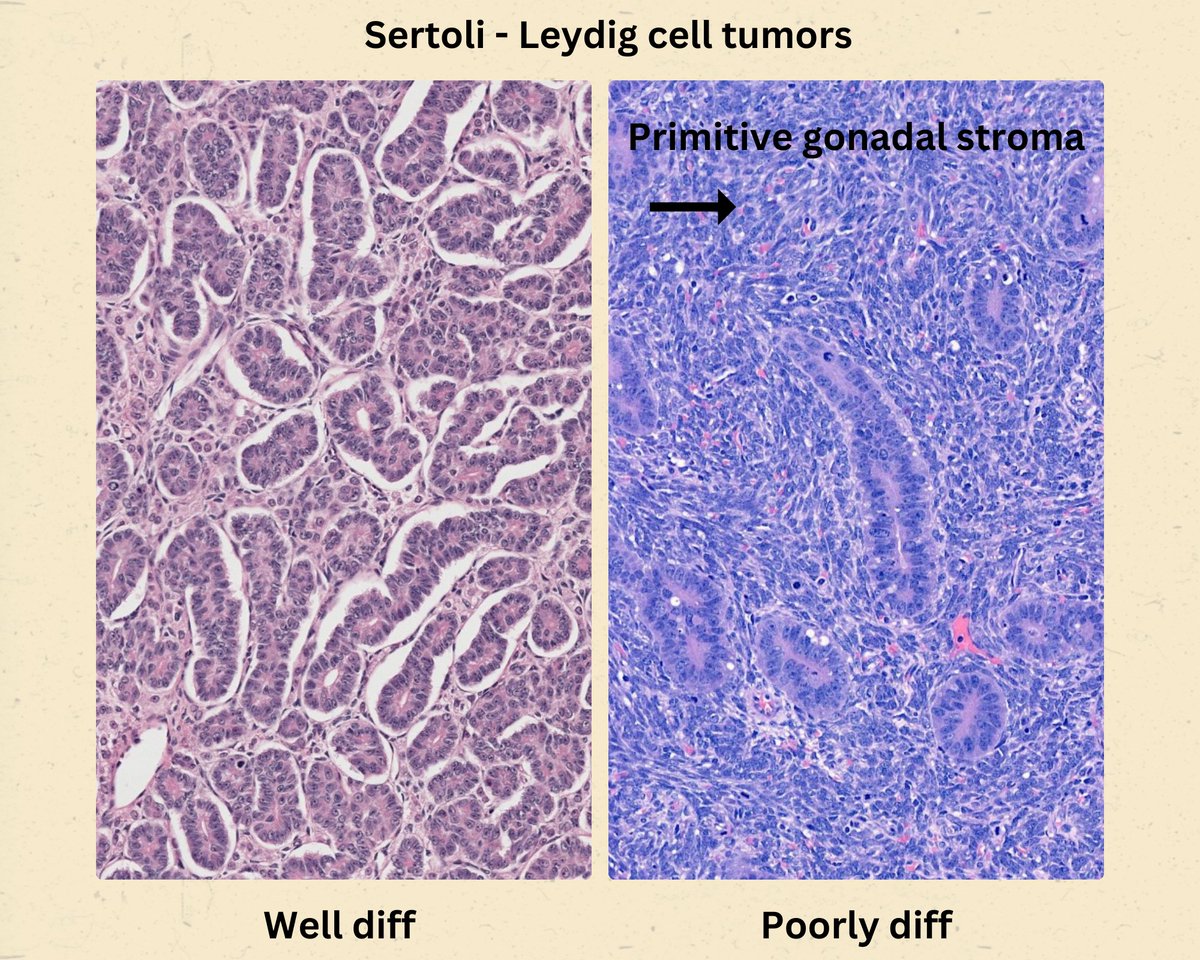
Ovary
Sertoli-Leydig cell tumor
Grade of differentiation
-Tubular differentiation of the Sertoli cell component (decreasing with increasing grade)
-Quantity of primitive gonadal stroma (increasing with increasing grade)
-Leydig cells also decrease with increasing grade
WHO and DAPA GR #EverydayGYN #gynpath #PathTwitter #pathologists #pathresidents #pathfellow
English