Angehefteter Tweet

Hey #medtwitter
Here are the basics on unequal randomization in trials
Why should we do 1:1 instead of 2:1 or 3:1 in phase 3 RCTs?
🧵
English
Vivek Patel, MD
312 posts

@vpatelmd
Assistant Professor @VUMCHemOnc | Co-Host @TheFellowOnCall | Alum of @VUMCMedicineRes @VUMedicine @dukeu | #meded #cancer | Tweets my own


Treatment Algorithm series: CLL with @mshadman ✅ Work-up ✅ Fixed duration Rx vs Continuous BTKi ✅ Role of antiCD20 w/ BTKi? ✅ Refractory disease Full discussion: - oncbrothers.com/algorithm-cll-… - Also on the “Oncology Brothers” podcast #HemeTwitter #OncTwitter @OncUpdates








Results GHSG HD21 BrECADD v eBEACOPP in 1L cHL #ASCO24: - 1500 pts, med age 31, Stage IIB 17%, rest adv stage - PFS superior in BrE arm: 4 yr 94% vs 91% (!!!) - less tox & neuropathy with BrE - 96% gonadal recovery with BrE (73% with escB) New standard of care in cHL? #lymsm
Congratulations to this year's class of Conquer Cancer Grant and Award recipients! We can't wait to celebrate with you at #ASCO24! Full list of recipients: brnw.ch/21wKdIf







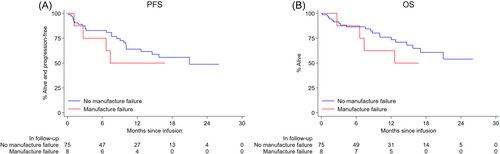
A very important study with policy solutions needed: insurance processes delaying CAR T infusions is bad news for patients! Looking forward to moderating this session. cc @vpatelmd @amarkelkar @ASH_hematology