Paul F. Austin@PaulAustin3w
We've been prescribing the same class of antidepressant for 40 years.
Two doses of psilocybin outperformed six weeks of it on nearly every measure that actually matters for living a full life.
In 2021, Robin Carhart-Harris's lab published what may be the most important depression study of the decade in the New England Journal of Medicine.
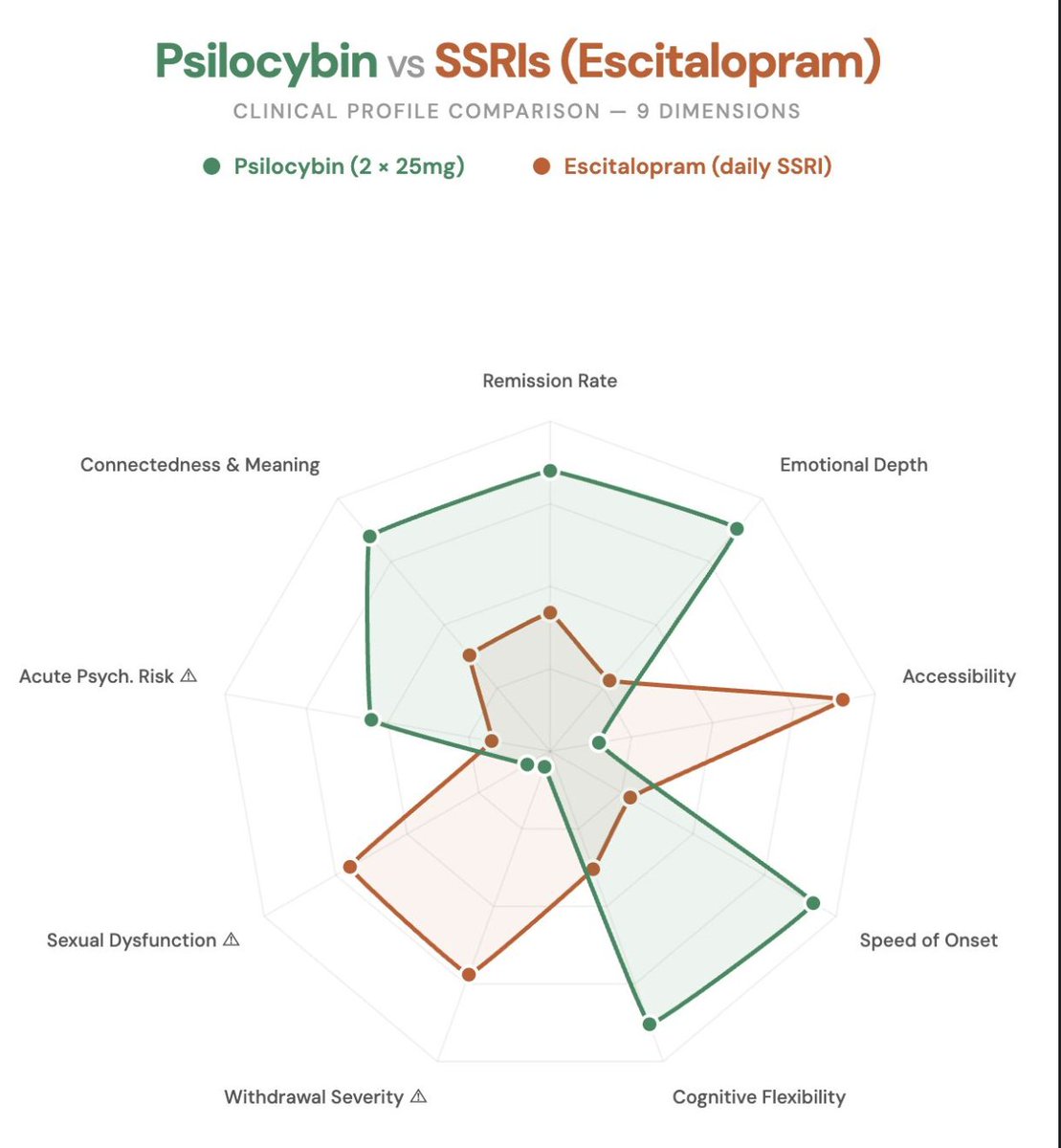
A head-to-head comparison of psilocybin therapy vs. escitalopram (a leading SSRI) for major depressive disorder.
Two doses of psilocybin (25mg, 3 weeks apart) vs. 6 weeks of daily escitalopram. Both groups received identical psychological support.
On the primary measure, the scores looked comparable. Headlines called it a tie.
But that's where most people stopped reading.
The secondary outcomes tell a radically different story:
→ 57% remission with psilocybin vs. 28% with escitalopram
→ 70% response rate vs. 48%
→ Psilocybin improved emotional depth; SSRIs blunted it.
→ Psilocybin preserved sexual function, SSRIs impaired it.
Two sessions. No daily pills, no withdrawals, and no sexual dysfunction.
The 6-month follow-up (Erritzoe et al., 2024) confirmed it. Psilocybin showed significantly greater sustained improvements in social functioning, connectedness, and meaning in life.
Not just fewer symptoms but a fundamentally richer experience of being alive (which is what we're all after, if I'm not mistaken).
The neuroimaging explains why. Daws et al. (2022) found psilocybin produced a global increase in brain network integration. The brain became more connected. Escitalopram showed no such change.
SSRIs turn down the volume on suffering. But they don't change the song.
Psilocybin disrupts rigid neural patterns, increases flexibility in brain networks, and as Dölen's research shows, reopens critical learning windows that allow new behavioral patterns to take root.
The SSRI model suppresses symptoms indefinitely. The psilocybin model opens a neuroplastic window, allowing for rewiring and a reintegration of hemispheric balance.
That's symptom management vs. actual transformation.
It's why we built our Practitioner Training at PCI the way we did. If psilocybin opens a neuroplastic window, the practitioner's job is to help clients make the most of it before it closes. Mapping protocols to neuroplasticity timelines while tracking relational & physiological change.
Our next Practitioner Certification cohort kicks off on February 19. I've dropped the link in the comments below if you want to learn more.
What are your thoughts on the future of depression treatment beyond the SSRI paradigm? How quickly do you believe psilocybin will take over as the first line of treatment for the majority of providers?
I'll share my guess in the thread below 👇