Chi Chu
2.4K posts


Chi Chu
@cdchu
nephrologist & descriptivist. #NSMC | epidemiology | clinical reasoning
San Francisco, CA Se unió Temmuz 2010
2.1K Siguiendo939 Seguidores
Chi Chu retuiteado

English gets its adjective endings -al and -ar (as in 'nasal' and 'lunar') from Latin -ālis and -āris.
These are really the same ending! Latin used the form -āris to avoid two Ls close together in a word.
Hence we find -ar in words with L in the root, like 'solar' and 'vulgar'.
English
@JohnRMontford @SegalMin @NephroGuy I see that perspective of unitlessness but it's a limiting view-the concept of units still makes perfect sense & is much more explanatory if broadened to be "g of _"
Esp helpful in conversions like K/Cr. The 0.113 mmol/g factor only cancels mmol or g of Cr not just any mmol…
GIF
English

@SegalMin @NephroGuy From a chemistry perspective (disclaimer: not a chemist) once you make a fraction of the same units they cancel and become dimensionless. That they are different substances shouldn’t matter. Maybe similar to a mass fraction of a whole? though that’s slightly different.

English
Spot urinary Pr:Cr are unitless dimensions, but I don't think wise to communicate as such.
"the uPCR is 5"
"the uACR is 300"
When questioned, the learner often cannot articulate WHY it is dimensionless. Let them express in: g/g or mg/g. Then the teaching can begin! #Nephpearls
English
@AlanYuNeph @JohnRMontford Exactly… even g/g does not cancel out. It’s g protein / g Cr
English

@JohnRMontford I don't think the concept of being dimensionless is helpful. I always remind learners to specify the units. A ratio in g/g is completely different from mol/mol (commonly used outside the US for Ca/Cr or K/Cr etc), for example.
English
@eugelin06 @NavTangri @NephroNinja @eric_weinhandl @hswapnil @ADAlthousePhD Could consider adding stepwise (have eGFR in model, then add eGFR slope) and seeing if overall fit improves, and argue if eGFR slope adds prognostic info. But effect sizes would not be cleanly interpretable. Teasing each apart w/collinearity is a conceptual challenge too IMO☝️
English

@NavTangri @NephroNinja @eric_weinhandl @cdchu @hswapnil @ADAlthousePhD Software considerations aside, if the variables are truly not orthogonal this isn’t necessarily a statistical problem, but a problem with the conceptual model right?
Alternatively if you’re in the business of prediction, you can let a ML model choose the variables for you?
English

Let's say variable x is strongly associated with the outcome and variable y is completely colinear with x (e.g., y = x + 10). If you run a Cox regression with x and y in the model, how does the model determine which variable (x or y) is independently associated with the outcome?
English
@MatthiasDiebold @hswapnil How much other IVF is there? Citrate rate?
Would look at total ins/effluent flow—if there’s lots (300+ ml/h) of 0K ins (citrate, drips etc), then maybe 3.2 is the steady state K…
Same principle as running D5 to reduce “effective” dialysate Na for CRRT+hyponatremia
@galindozip
English

@hswapnil He is on 3-7mcg/min NE. I measured the K+ from the drainage. It was 2.7 mmol/l. I went so far as to measure the K+ in the dialysate which was 4mmol/l as it is supposed to be. I believe it has to be a shift but I am not sure what causes it?
English
Pat w/ duodenal perf + septic shock, RRT anuric. Persistent hypokalemia of 3.2mmol/l after 48h with dialysate K+: 4mmol. Postfilter K+ 3.2mmol. No drugs for shift. cvvHDF w/ citrate Qb 150, Qd 1500, UF 50 Fluid loss via drainage 500ml/d from perforation site. Any ideas? #askrenal
English
@NephroGuy @Yahyaraufahmad @kidney_boy Last step should be (if you want to BSA index) to multiply by 1.73 then divide by the person’s BSA
So if the BSA is 3.46 (roughly double), then CL is only 41*1.73/3.46 = 20 ml/min per 1.73m2
For 1.73m2 person with 41 ml/min GFR, the indexed = 41 ml/min/1.73m2 (as it should be)
English
What is the approximate effective GFR of a patient on continuous renal replacement therapy with therapy fluid at 25 ml/kg and UF of 100/hour? #AskRENAL
English
@rabihmgeha @DxRxEdu 'triphasic' response with hypothalamic tract surgery/trauma comes to mind:
1) hypothalamic dysfunction ➡️ DI
2) pituitary degeneration & ADH release ➡️ SIADH
3) depletion of ADH stores ➡️ DI
ncbi.nlm.nih.gov/pmc/articles/P…
pubmed.ncbi.nlm.nih.gov/16700319/
English

One example -
Insulin antibody syndrome can result in both HYPO and HYPERglycemia.
Can you think of other examples, #medtwitter?
<3 @DxRxEdu
English
The goal of treatment is restore a physiologic balance go awry.
Hyponatremia -> Normal sodium
Occasionally, we accidentally over do it.
Less frequently, the disease spontaneously swings from one extreme to another
English
@Nephro_Sparks @ClementLeeMD @hswapnil @ssfarouk @PAWellingMD And also plug for superhero kidney physiology as a future #nephmadness region
English

English

Why can’t the human kidney excrete free water without solutes? Is it because that level of hypoosmolality can cause hemolysis? Is it because it would be too energy-dependent? Is there a teleological argument? #askrenal @TimRowesays @ShreyaTrivediMD
English
@Nephro_Sparks @ClementLeeMD @hswapnil @ssfarouk @PAWellingMD Yes—the animals nicely represent extremes. There are always limits, but it is interesting to wonder why physiology has these limits (even/especially in animals that push them to the extreme)
English
@cdchu @ClementLeeMD @hswapnil @ssfarouk @PAWellingMD I interpreted his question in that we are very reliant on solute. Which indeed we are as humans.
English
@Nephro_Sparks @ClementLeeMD @hswapnil @ssfarouk @PAWellingMD Right I interpreted the question as making *pure* water—not just low osm, 0 osm. But does any animal do this?
(Although I think the need is not there. Even a freshwater fish has osms it needs to excrete)
English
@cdchu @ClementLeeMD @hswapnil @ssfarouk @PAWellingMD That’s not necessarily true. If the argument is teleological it’s all about design and need. A different design… say the kidney of a freshwater fish is able to produce urine with a consistent osm of less than 50. So human kidney designed differently
English
@ClementLeeMD @Nephro_Sparks @hswapnil @ssfarouk there’s some misinterpretation of the question, by free water I think you mean water with 0 osmolality. “Free water” is a sort of theoretical/relative concept (we do excrete FW regularly)
See @PAWellingMD answer re: energy. Need to maintain huge gradients to make pure water
English
@Nephro_Sparks @hswapnil @ssfarouk Thanks Matt. However-- why not? Why does the human kidney not have a mechanism for excreting free water? Theoretically we could have ATP pumps that can use energy to rid free water, right? Wouldn't that be useful for hyponatremia, such a common problem?
English
@SatyaPatelMD Do you mean meds that can ⬆️ Cr without GFR change (bactrim, dolutegravir etc)
Or meds that can ⬆️ Cr, truly reduce GFR, but without intrinsic injury? (ACE/ARB, SGLT2i)
IMO, rampant Cr criticism (albeit deserved) distracts from the reality that not all true GFR reduction is bad
English
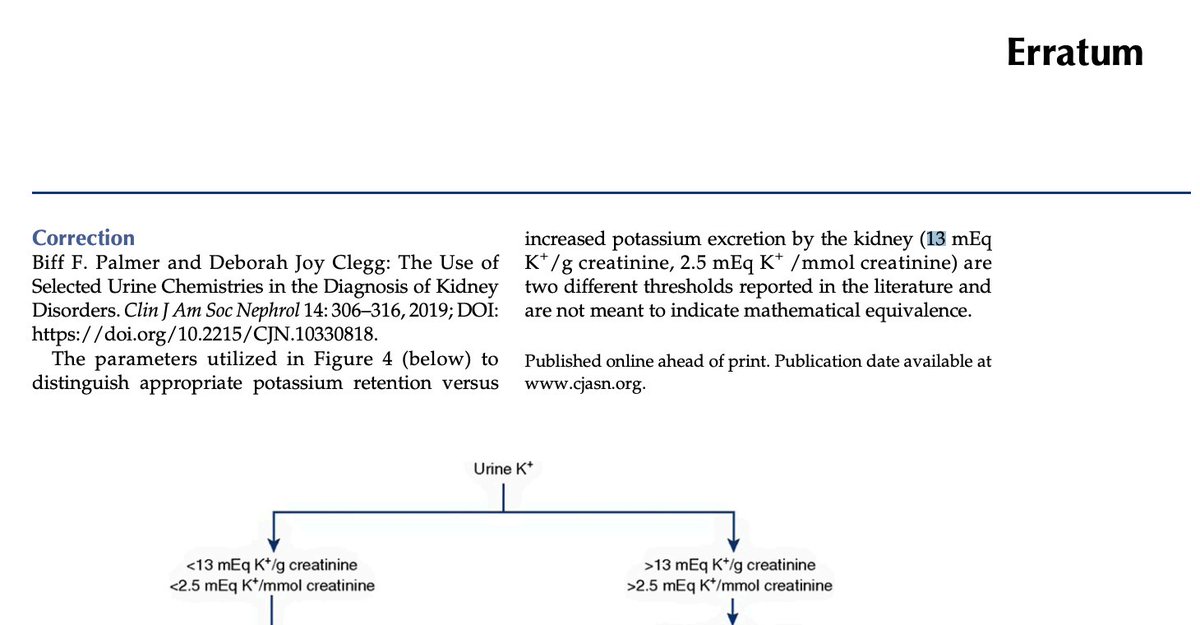
@NephroMD @kdjhaveri @AlanYuNeph @purvasharma821 Also in this figure, there's a correction to clarify 13 meq/g is not the same as 2.5 mmol/mmol, they are thresholds from different sources (no citations). That was always a source of confusion with this algorithm...
English

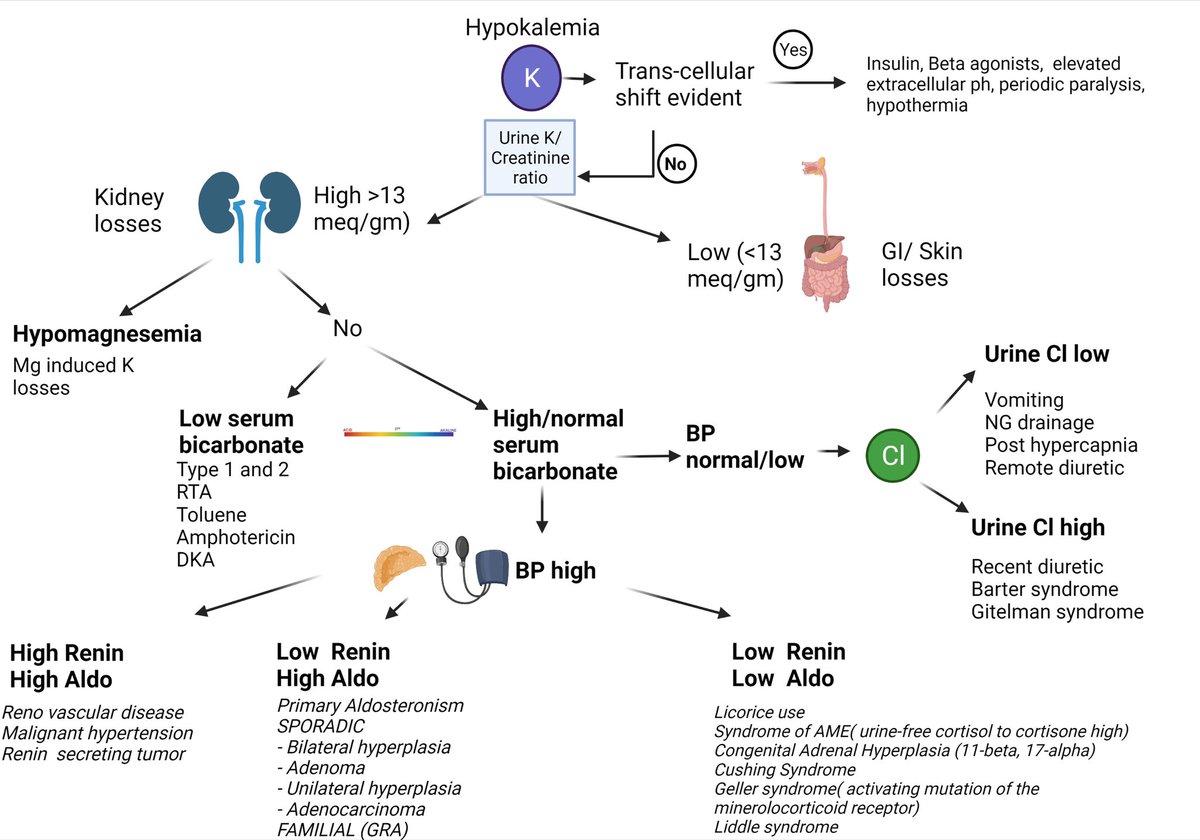
nephronpower.com/2022/05/concep… #nephronpower #conceptmap on hypokalemia and HTN @NephroMD @purvasharma821
English
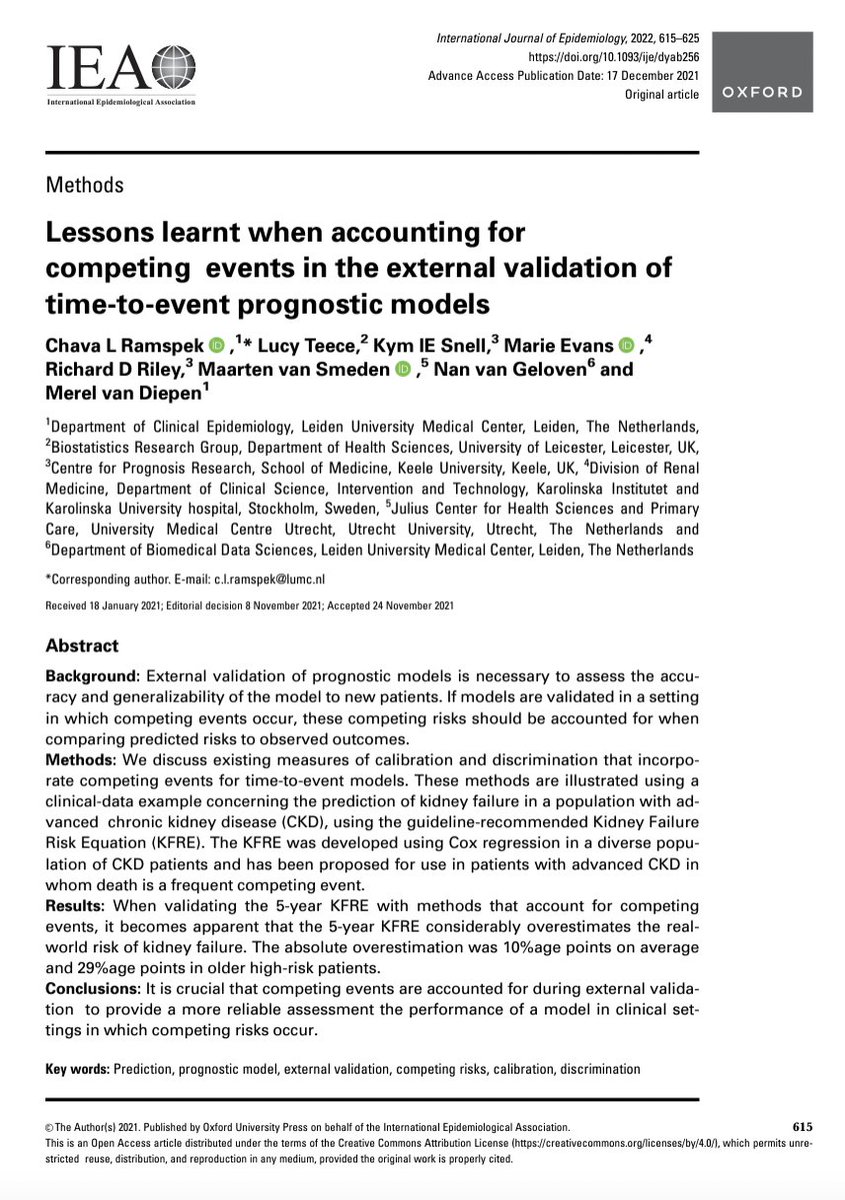
@NavTangri @AdanZBecerra1 @MaartenvSmeden @IntJEpidemiol @ramspek @LucyTeece @Kym_Snell @Richard_D_Riley @GelovenNan Agree @NavTangri. & in very high risk where gross miscalibration occurs (50% vs 80% sounds like/is a big error), at least for KFRE, it's clinically obvious both are very near ESKD. Clinical decisions aren't really different & death is a consideration on top of KFRE either way.
English

@AdanZBecerra1 @MaartenvSmeden @IntJEpidemiol @ramspek @LucyTeece @Kym_Snell @Richard_D_Riley @GelovenNan So - my view is
Competing risk a real problem in late stage CKD in high risk older adults at 5 years
However, in late stage CKD in high risk older adults, you are usually making decisions (fistula etc) on 2 year risk, where competing risk doesnt really matter
English

Now published @IntJEpidemiol: why and how to deal with competing events when performing the validation of a prediction model
doi.org/10.1093/ije/dy…
English
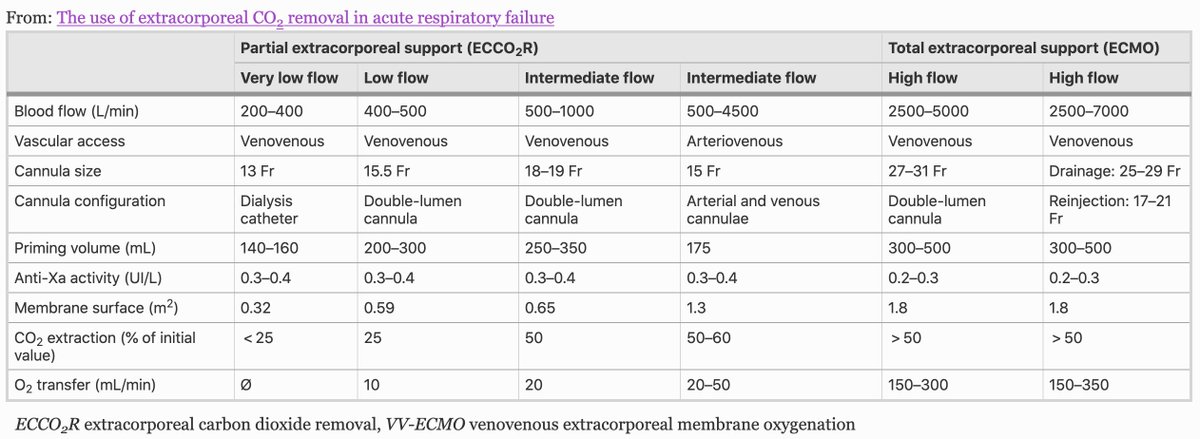
@jaykoyner @NephRodby @lowgfrdoc @DrTomasGuerrero @hswapnil @kdjhaveri @edgarvlermamd @kidney_boy @AmandaDZeidman From Table 1 in the article: In-line CO2 removal with CVVH (considered "very low flow") - has been tried but not very effective. Can get CO-level Qb with ECMO (which is pretty much air/gas dialysis).
annalsofintensivecare.springeropen.com/articles/10.11…
English

@NephRodby @lowgfrdoc @DrTomasGuerrero @hswapnil @kdjhaveri @edgarvlermamd @kidney_boy @AmandaDZeidman @nkf @Lucas_Kimmig I meant a normal renal blood flow is 1200ml/min
So the ratio of normal to replacement flow is not 1:1.
So don’t need to replace pulmonary flow in a 1:1 fashion
Chicago, IL 🇺🇸 English

#ask renal Do you do extra corporeal Co2 removal by hemodialysis at your center or any suggestions/comment?
@hswapnil @kdjhaveri @NephRodby @edgarvlermamd @jaykoyner @kidney_boy
English
@NavTangri @Jwaitz @egottliebMD When diff isn't big, answer is likely in btwn (combined eqn).
I'm tempted to think in wide disagreement, the likely case is at least 1 is being thrown off by non-GFR factors, and truth isn't necessarily the middle. But hard to know, and middle still may be best guess on average.
English
@Jwaitz @egottliebMD I would say true egfr is probably closer to the middle in this patient and I end up using the combined equation when I have both measurements available. I have def seen measurements this far apart
English

How different is the most different you've ever seen between a creatinine-based eGFR and a cystatin c-based eGFR? If one is 60 and the other 25, which one should I believe? Is splitting the baby (cys-creat eq) really the right call? #askrenal
English
@RahulM_MD Perhaps partly counteracted by Gibbs-Donnan effect, but I think mild hyponatremia is not uncommon on CRRT... @hswapnil
twitter.com/hswapnil/statu…
Swapnil Hiremath @hswapnil.medsky.social@hswapnil
@NephRodby @amolmpatel @DCharytan @kidney_boy @jaykoyner @edgarvlermamd nice - really useful review - relevant snippet below We went down this rabbit hole few years ago while measuring dialysate sodium - kireports.org/article/S2468-… in @KIReports - make sure one uses the correct conversion factors if doing so!
English

If plasma free water sodium concentration is 154, why don't HD and CRRT with dialysate/replacement fluid sodium concentrations of 140 cause hyponatremia?
#askrenal
English
@NephRodby Have spent so much time chasing literature on the “descending limb”. Despite how ubiquitous “falling off the Starling curve” is as a colloquialism in wards teaching. Still don’t have satisfactory answers… @JGAmatruda
English

One of my favorite things to draw on rounds! I do discuss the controversy of extending it to the right going downward, CO starting to fall if LVEDP gets too high. Cardiologists hate me for that, but I'm not convinced that "downside of the Starling curve" exists or doesn't.
NephroPOCUS@NephroP
When the 🫀is operating on the steep portion of Frank-starling curve, stroke volume (SV) ⬆️ substantially when preload is ⬆️ with IV fluids; when 🫀is on flat portion, further ⬆️ preload will not substantially ⬆️ SV. + response varies from pt to pt 👇 #POCUS #MedEd #Nephrology
English
@Jwaitz @Gabby_Brauner27 Creatinine is not great, but everything you said is true even if we had a perfect GFR test. I tend to think of ACEi/ARBs as negative GFR-tropes (definitely not "nephrotoxins"). Imagine if people labeled beta blockers cardiotoxins😬...but here we are.
#lowpowermode
English
@Gabby_Brauner27 In short,
-ACEis and ARBs are great
-creatinine and skittish nephrologists are not great
-Textbooks/review books need an update
-Don’t fear the creatinine reaper
(11/11–Fin)
GIF
English

I'm confused about ACEi re: diabetes and kidney disease. ACEi are protective of kidneys in a patient with HTN and DM, but can worsen kidney failure in a patient already with diabetic kidney disease? I'll try to do some reading on this tomorrow, but twitter is easier 😂
English