Sabitlenmiş Tweet

Excited to share our paper, now out in @JACCJournals! Important work led by @MAlvarezVillela:
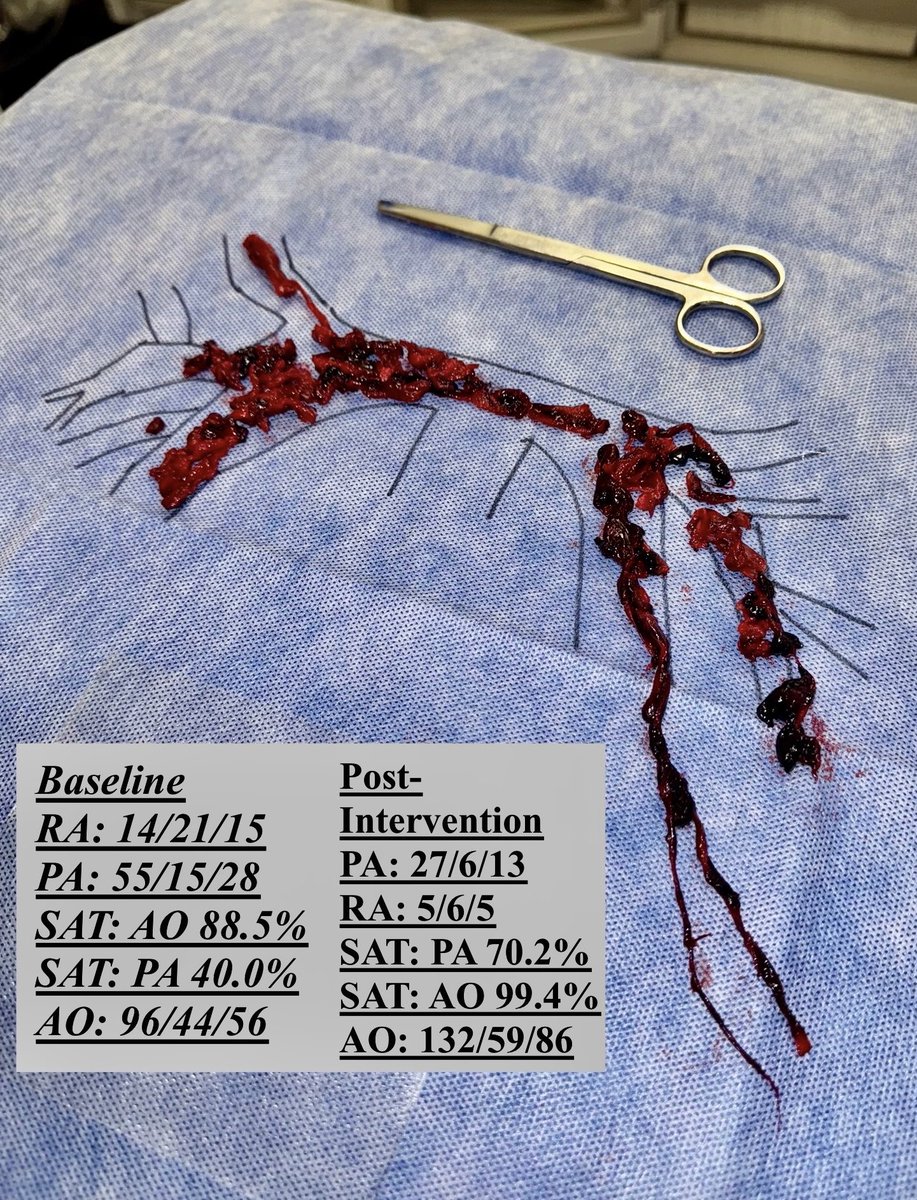
🔥 Fever in AMI-CS is common and is associated with greater illness severity but seems to be noninfectious in most cases
#CardiogenicShock 🫀
doi.org/10.1016/j.jaca…

English