
Tom Wilson
2.3K posts
Tom Wilson
@TWilsonMD
Interventional Cardiologist, CTO-PCI, CHIP, Peripheral vascular disease, acute PE. Views & opinions are my own.
Rapid City, SD Katılım Şubat 2021
368 Takip Edilen1K Takipçiler

Curious to hear opinions: 99F s/p TAVI (Allegra 23) developed CAVB ~2h post-procedure that resolved within ~1 hour. Would you proceed with PPM implantation or watchful waiting?
English
@ColletCarlos @rotamonster PCCTA will be ready for us to use in 2-3m. Is high iodine contrast a must have or does 350 do the job? What do you use?
English

Very soon, we will be assessing PCI results with non-invasive imaging.
This case shows a left main crossover PCI to the LAD, where our main question was the result at the ostium of the circumflex.
#CCTA will rapidly become an important tool not only for planning PCI, but also for evaluating its final result.
@crfheart @PCRonline @SCAI @Heartflow @ACCinTouch @JACCJournals @ESC_Journals
English
@Hragy @jedicath @djc795 @DrRajeshG1 @SyedYNaqvi1 @KPujdak @DocSavageTJU @DMemmini @IntervnCardio @realarainmd @SrihariNaiduMD @cingolani_oscar @BaoGTran @DrRajeshG1 PCI of anomalous RCA off mLAD. Severe focal Ca, **Ca fracture, 3.5mm DES post 4.0 to 20 atm.
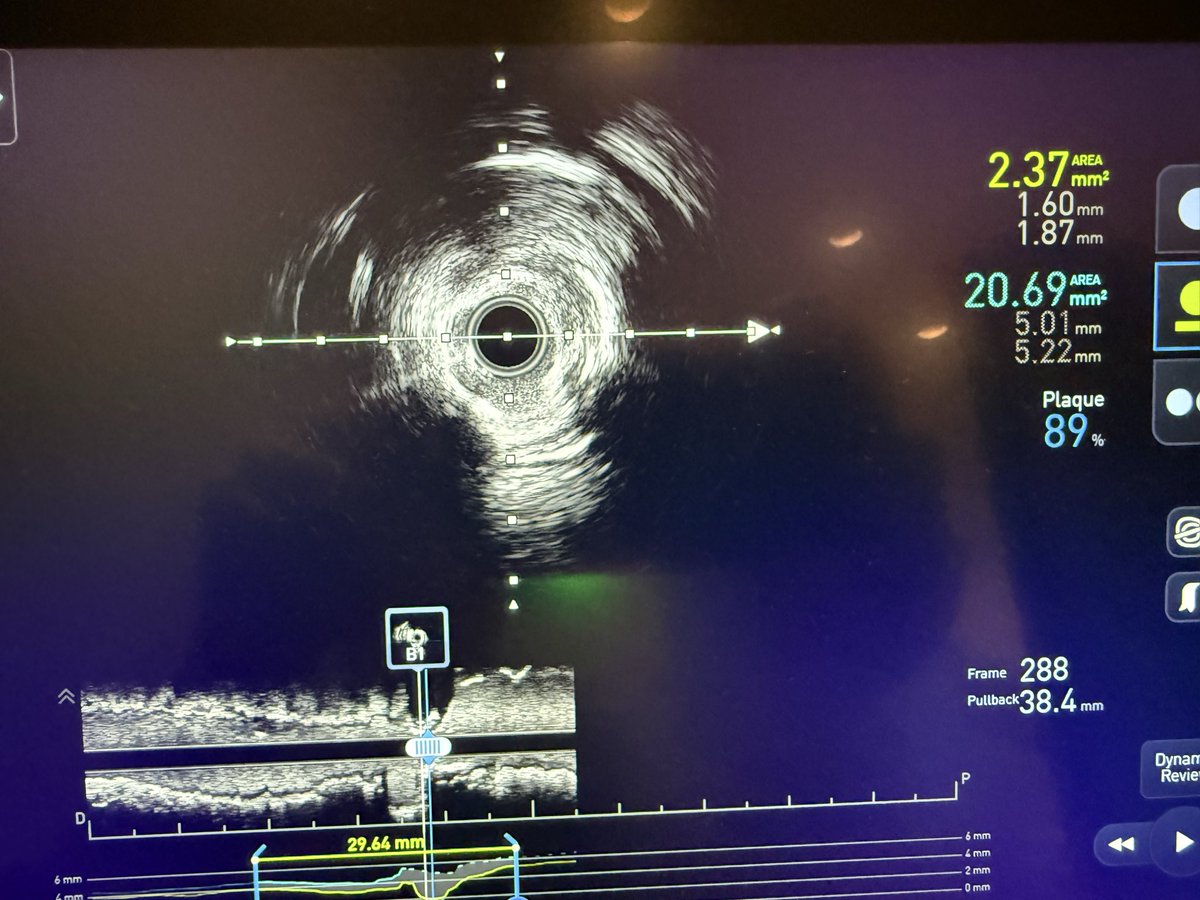

English
@Hragy My Answer: call the referring doc. Have a discussion. Maybe the patient has been symptomatic. If not, discuss option for Rx therapy, close follow up.
English

@TWilsonMD @Hragy I think that’s the same phenomenon. It leads to an unnecessary stress test, which then leads to an unnecessary cath, etc, etc,
English
@DMemmini @BaoGTran @realarainmd @DrJayMohan @KPujdak @DrRajeshG1 @SrihariNaiduMD @MichaelMegalyMD @djc795 @jl35wilsonMD @rational_doc Wow! Will send final angio when able.
English

@TWilsonMD @BaoGTran @realarainmd @DrJayMohan @KPujdak @DrRajeshG1 @SrihariNaiduMD @MichaelMegalyMD @djc795 @jl35wilsonMD @rational_doc I have been looking at angios since 1987 and have never seen this before. Very cool.
English
@realarainmd @DrJayMohan @KPujdak @DrRajeshG1 @SrihariNaiduMD @MichaelMegalyMD @djc795 @jl35wilsonMD @rational_doc how many times have you seen this variant? 1,0,0 LAD-RCA lesion!
English
I didn’t advocate for 1 size fits all and never would. I referenced DCBs and BVS, to severely limit permanent implants in coronary arteries, especially younger patients or HBR. DES will be around for decades-just want to decrease use if able. Being skilled w multiple tools is vital.
English

@Hragy @TWilsonMD What do you think is the motivator for "one approach fits all"?
Is it corporate greed, or physician need to have a preferred tool that they can use in 95% of cases?
Aiming for particular niche with unmet need doesn't seem like a bad idea, build out from that bridgehead later??
English

Anyone who worked as an interventional cardiologist before the introduction of Stents , knows that the current direction to promote DCB as stent free PCI world will fail.
What we really need to know is if we can use DCB when and where we do not want to put DES,like distal LAD.
English
@IntervnCardio @realarainmd @DrJayMohan @KPujdak @DrRajeshG1 @SrihariNaiduMD @MichaelMegalyMD @djc795 @jl35wilsonMD @rational_doc Would be great to see thank you for looking.
English

@TWilsonMD @realarainmd @DrJayMohan @KPujdak @DrRajeshG1 @SrihariNaiduMD @MichaelMegalyMD @djc795 @jl35wilsonMD @rational_doc Had seen exactly same anatomy around 10 years back, will try to hunt the images
English
@DrAnkushG @BaoGTran @realarainmd @DrJayMohan @KPujdak @DrRajeshG1 @SrihariNaiduMD @MichaelMegalyMD @djc795 @jl35wilsonMD @rational_doc Very nicely done. Thank you for sharing.
English

@TWilsonMD @BaoGTran @realarainmd @DrJayMohan @KPujdak @DrRajeshG1 @SrihariNaiduMD @MichaelMegalyMD @djc795 @jl35wilsonMD @rational_doc academic.oup.com/ehjcr/article/…
Had one patient with same anatomy, first did PCI to prox LAD with rota before origin of RCA, came back with ACS with persistent ISR then did LAD/RCA bifurcation angioplasty. 6.5 yrs clinical follow up- doing fine
English
@realarainmd @DrJayMohan @KPujdak @DrRajeshG1 @SrihariNaiduMD @MichaelMegalyMD @djc795 @jl35wilsonMD @rational_doc I do—just not at the ready.
English

@TWilsonMD @DrJayMohan @KPujdak @DrRajeshG1 @SrihariNaiduMD @MichaelMegalyMD @djc795 @jl35wilsonMD @rational_doc Very nice1 I am seeing this configuration for the first time. Do you have other views?
English
@BaoGTran @realarainmd @DrJayMohan @KPujdak @DrRajeshG1 @SrihariNaiduMD @MichaelMegalyMD @djc795 @jl35wilsonMD @rational_doc I had to blink twice to make sure my eyes were telling me what I thought I was seeing!
English

@TWilsonMD @realarainmd @DrJayMohan @KPujdak @DrRajeshG1 @SrihariNaiduMD @MichaelMegalyMD @djc795 @jl35wilsonMD @rational_doc Crazy. Would love to see more views and maybe a CTA.
So the “RCA” wraps over the RV? It doesn’t look like an interarterial coarse but I can’t be sure
English
@BaoGTran @realarainmd @DrJayMohan @KPujdak @DrRajeshG1 @SrihariNaiduMD @MichaelMegalyMD @djc795 @jl35wilsonMD @rational_doc Appears to be nowhere near an interarterial course based on angio. I should have snapped more views. Photon counting CTA available next door soon.
English
@aspergian1 @realarainmd @DrJayMohan @KPujdak @DrRajeshG1 @SrihariNaiduMD @MichaelMegalyMD @djc795 @jl35wilsonMD @rational_doc Same. What a great spot for a big ‘ol stent.
English

@DrRajeshG1 @realarainmd @DrJayMohan @KPujdak @SrihariNaiduMD @MichaelMegalyMD @djc795 @jl35wilsonMD @rational_doc What an honor! Making the charts on Dr. G’s board!
English

@TWilsonMD @realarainmd @DrJayMohan @KPujdak @SrihariNaiduMD @MichaelMegalyMD @djc795 @jl35wilsonMD @rational_doc Only once in my 28 yr service
English
Tom Wilson retweetledi

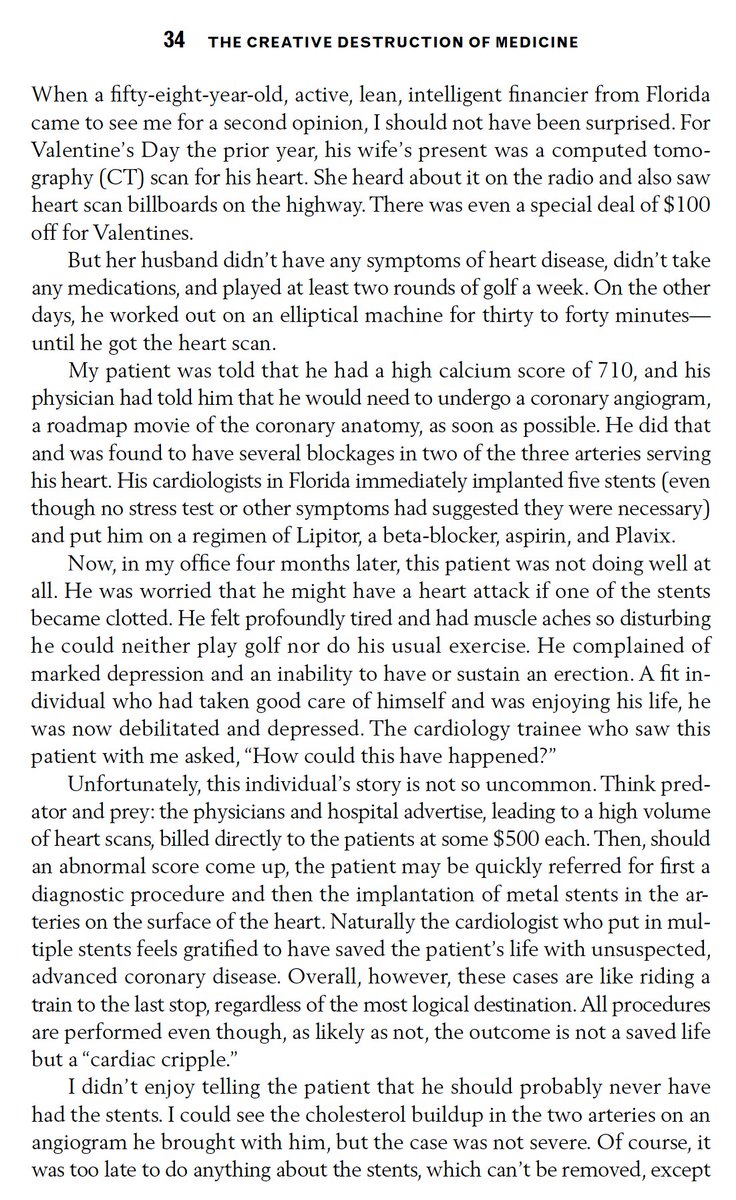
@drjohnm I have been outspoken on the massive misuse of CAC testing for a long time (excerpt from my book in 2011) and have never ordered one.
English

@georgetolisjr Oh u need to see interventional meetings. It’s even worse there
English
Cardiac surgical societies should require all “experts” to turn in a case list before they can sit on a national meeting panel and lecture the audience about “how I do it” or “how I teach it”.
English
@IR_Doctor @t_intheleadcoat @farkomd @_backtable @JayMathewsMD @DrRajeshG1 @KPujdak @realarainmd @cardiojaydoc02 @SripalBangalore More gnar here than any mtn in America
English

@t_intheleadcoat @TWilsonMD @farkomd @_backtable @JayMathewsMD @DrRajeshG1 @KPujdak @realarainmd @cardiojaydoc02 @SripalBangalore Agree. Serious gnar in thar.
English
@farkomd @_backtable @JayMathewsMD @DrRajeshG1 @KPujdak @realarainmd @cardiojaydoc02 @SripalBangalore @IR_Doctor 70M, h/o SMA aneurysm w surg repair x2 (2010/18) at tertiary care center. Back w ASx enlarging SMA aneurysm. Next step? Pt has not done well w/ Surgery. Endo option?

English