Sabitlenmiş Tweet

@MacEmergFRCPC congratulations & welcome to our newest member of the Mac Emerg residency program, born January 9th, 2024.

English
Ashley Lauren
3.3K posts

@ALubeyMD
ER MD Peel Region, @MacEmerg FRCPC 2020 & @UofTMDProgram 1T5 alumni. Clinician Educator DRCPSC.





BREAKING: The U.S. drops the number of vaccines it recommends for every child in an unprecedented overhaul of childhood health protections. apnews.com/article/childh…




Whooping cough cases soar as vaccination rates drop. nbcnews.com/health/kids-he…





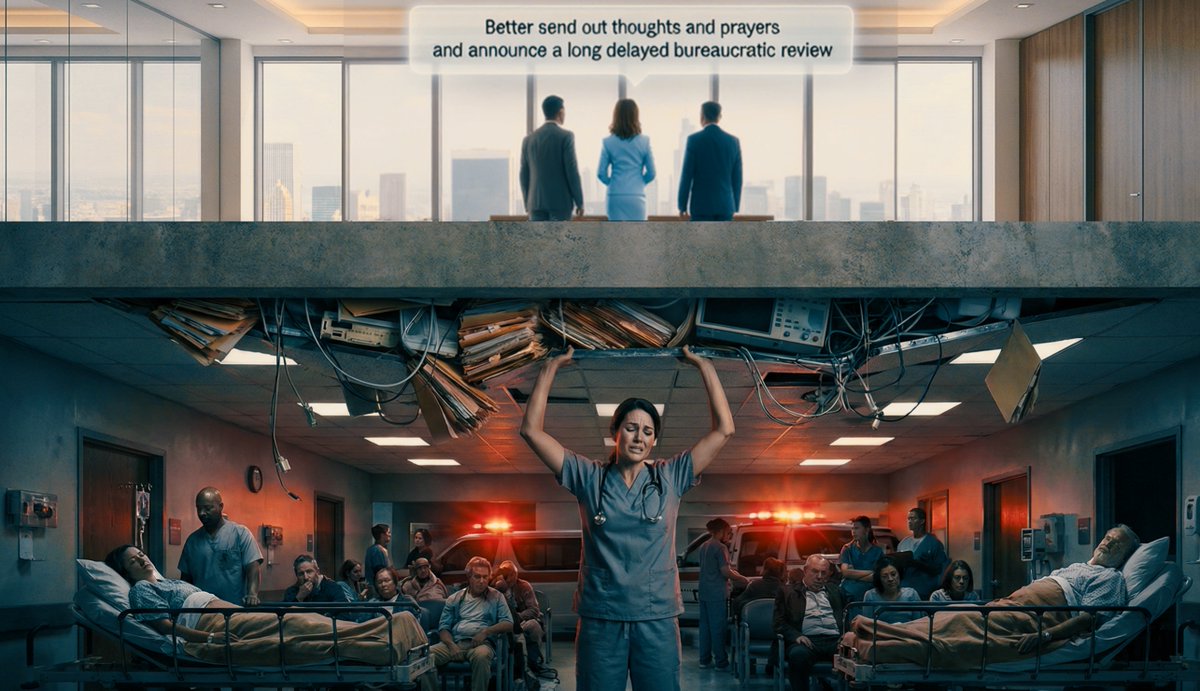
Just a reminder to all Albertans: we already cannot staff our large hospitals with Ultrasound Technicians to provide safe and timely care for all kinds of afterhours emergencies. buff.ly/ovAGkeq